
Shelly is back at it again, trying to get information from the regime of Robert Strang.
The latest find involves adverse effects and “messaging” that public officials are expected to undertake. It’s actually quite sickening to read it. Here is what was requested:
Amended September 21, 2022: Copies of all records such as correspondence (emails, and letters) reports and documents sent to/given to/ reported to/received by Dr. Robert Strang from doctors, pharmacies, medical officers, hospital administration, long term care and nursing home administration – on the topic of COVID-19 vaccine adverse events/side-effects and deaths that have occurred since it was rolled out in our province. This would include correspondence and reports on adverse events and deaths that are temporally associated with vaccine that have not been clearly attributed to other causes that Dr. Robert Strang has had in his possession. (Date Range for Record Search: amended to Dec 7, 2020-June 7, 2021)
However, sections of the release — and certain names — were redacted because:
- Section 14: advice by or for a public body or minister. 14(1): The head of a public body may refuse to disclose to an applicant information that would reveal advice, recommendations or draft regulations developed by or for a public body or a minister.
- Section 20: unreasonable invasion of personal privacy. 20(1): The head of a public body shall refuse to disclose personal information to an applicant if the disclosure would be an unreasonable invasion of a third party’s personal privacy.
Looking through the release package, there are other questions that need to be asked.
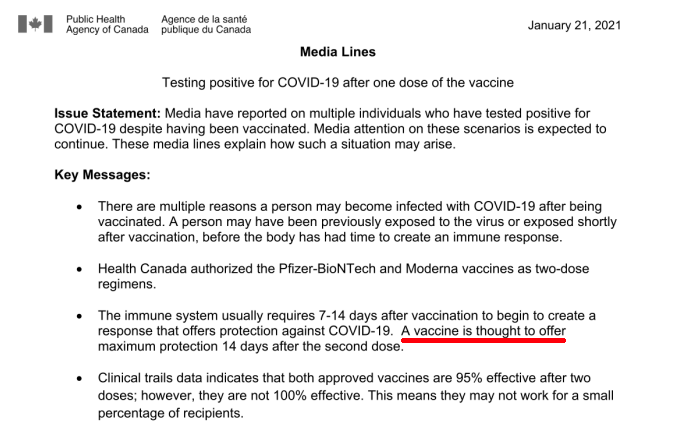
(On page 4) it states that “vaccines are thought to offer” maximum protection after 14 days. Perhaps this is overanalyzing, but it comes across as just guessing and speculation.
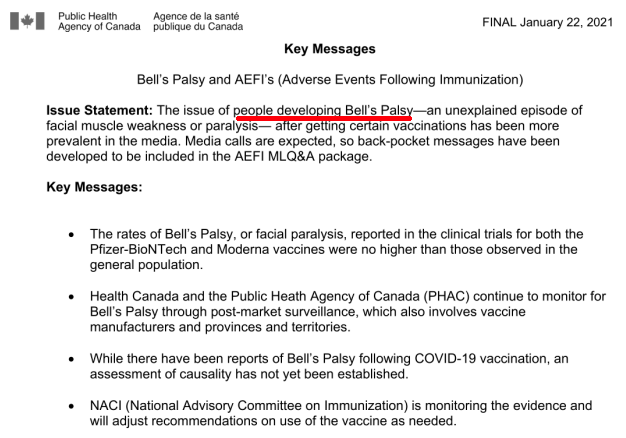
(On page 7) it was already being reported in January 2021 that people were getting Bell’s Palsy. Instead of pulling the vaccines, there was “messaging” underway to convince the public that it was no big deal.
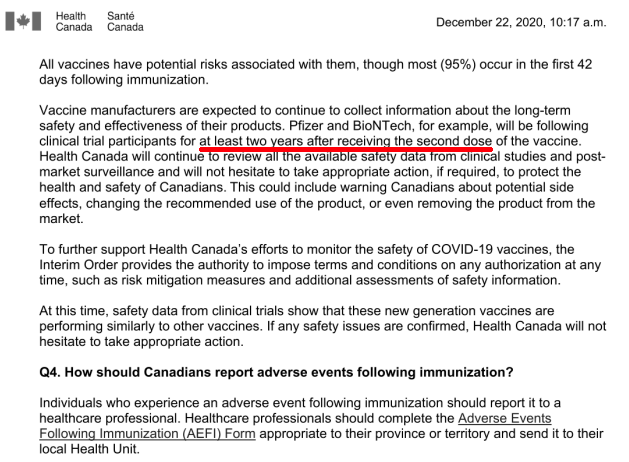
(On page 26) it’s tacitly admitted that they don’t have any long term data on their test subjects. Apparently, they are to be followed and monitored for 2 years after the fact. That’s fine on its own, but shouldn’t the lack of testing have been made public from the beginning?
If it wasn’t obvious already, officials in Nova Scotia are essentially actors reading from a script. They have been coached on what to say, and how to address inevitable concern from the public. Decide for yourself if this amounts to meaningful transparency.
A death due to COVID-19 is defined for surveillance purposes as a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma). There should be no period of complete recovery from COVID-19 between illness and death.
The bogus definition of a “covid death” has been covered here before. There’s no way to describe this other than as fraud.
There’s also this minor issue that this so-called virus has ever been proven to exist. If you haven’t yet seen Christine Massey’s work, it’s available online.
(1) 2022-01349-HEA Decision Letter Messaging
(2) 2022-01349-HEA Release Copy Messaging
(3) https://shellyhipson.ca
(4) https://www.fluoridefreepeel.ca/fois-reveal-that-health-science-institutions-around-the-world-have-no-record-of-sars-cov-2-isolation-purification/
OTHER ARTICLES BASED ON SHELLY’S FOIA WORK:
(1) https://canucklaw.ca/nova-scotia-foi-response-tacitly-admits-there-is-no-wave-of-hospitalizations/
(2) https://canucklaw.ca/nova-scotia-foi-result-province-refuses-to-turn-over-data-studies/
(3) https://canucklaw.ca/more-foi-requests-from-nova-scotia-trying-to-get-answers-on-this-pandemic/
(4) https://canucklaw.ca/nova-scotia-foi-request-shows-province-reduced-icu-capacity-in-recent-years/
(5) https://canucklaw.ca/nova-scotia-foi-shows-province-has-no-evidence-asymptomatic/
(6) https://canucklaw.ca/nova-scotia-foi-province-refuses-to-turn-over-contract/
(7) https://canucklaw.ca/nova-scotia-foi-19-1-million-spent-on/
(8) https://canucklaw.ca/nova-scotia-foi-no-real-increase-in-deaths-due-to-pandemic/
(9) https://canucklaw.ca/nova-scotia-foi-more-deaths-as-vaccination-numbers-climb/
(10) https://canucklaw.ca/nova-scotia-foi-govt-data-on-deaths-by-age-vaxx-status/
(11) https://canucklaw.ca/nova-scotia-foi-another-data-dump-on-cases-vaxx-rates/
(12) https://canucklaw.ca/nova-scotia-fois-miscellaneous-findings-on/
(13) https://canucklaw.ca/nova-scotia-foi-cant-be-bothered-with-pfizer-docs/
(14) https://canucklaw.ca/nova-scotia-foi-pfizer-docs-aefi-deaths-weather-modification/