

The Canadian Paediatric Society, or CPS, is a group that claims to be concerned with the health and well-being of young children. However, after looking at their website, there are grounds to be concerned. There is also a section on convincing children to wear masks, which is disturbing.
The CPS also pushes the racial justice narrative heavily, implying that tolerance and diversity will solve just about everything. Their Twitter account is full of this nonsense.
Particularly troubling is the “guidance” they gave out in September 2021, regarding myocarditis and pericarditis. These are serious side effects that can result — even in children — from taking the injections that the Government calls vaccines.
Abstract
This practice point aims to provide clinical guidance on myocarditis and pericarditis following mRNA COVID-19 vaccination (Pfizer-BioNTech and Moderna). The benefits of COVID-19 vaccination outweigh the risks, and the vaccine is recommended for all eligible individuals, including children and youth in their 12th year and over. A small increased risk of myocarditis and pericarditis (< 1 case per 10,000) has been reported following vaccination with COVID-19 mRNA vaccines in Canada and internationally, most often among adolescents and young adults < 30 years of age, males, and after the second dose. Although this safety signal is occurring at higher-than-expected background rates, most cases are mild. This document reflects expert opinion and available evidence, which is limited. It will be updated as further information becomes available and as younger individuals are immunized against COVID-19.
Myocarditis. In general, most reported cases of myocarditis following COVID-19 mRNA vaccination have been mild and have shown response to NSAIDs. However, admission or close ambulatory monitoring should be considered until the clinical course of the illness is established. Severe cases with heart failure, arrhythmia or other complications of myocarditis require hospitalization, critical care support with appropriate management and monitoring.
Conclusions
(1) There is a temporal association between receiving mRNA COVID-19 vaccination and myocarditis and pericarditis among youth. These events are very rare. The risk-benefit decision for mRNA vaccination is favourable, and the vaccine is recommended for all eligible populations.
(2) Clinical evaluation should be in person and include a history, physical examination, and investigations (ECG, serum troponin and inflammatory markers).
(3) Most cases are benign, respond rapidly to NSAIDs alone, and can be safely managed in the ambulatory setting.
(4) All suspected and confirmed cases should be reported to local/provincial or territorial public health authorities as Adverse Events Following Immunization (AEFI)
Do you have any concerns over reports of myocarditis and pericarditis from people who’ve take the so-called vaccine? Don’t worry, it’s apparently nothing to be worried about.
In fairness, it’s a bit unclear whether this is the CPS’ official position, or just the work of contributors they published. Either way, it’s disturbing.
In their (now removed or relocated) policy position, the CPS references to myocarditis and pericarditis issues and seems to recommend the vaccines to children anyway. They do recommend these diagnoses be reported, however.
The CPS acknowledges that these “vaccines” could be causing heart problems, including in children. This group STILL recommends that kids get them. One has to wonder if there is more to this than meets the eye. Readers of this site will immediately suspect that some money has changed hands.
And yes, the answer is always the same. This “independent” group has been getting funds from entities that have an interest in pushing certain narratives.

According to their profile with the Federal Government, the CPS is looking at: “Expanding access to paediatric medications and therapeutics through federal legislation, regulatory and policy change”. In practical terms, this means pushing for ever greater influence of big pharma, even onto young children.
| GOVERNMENT DEPARTMENT | YEAR | MONEY |
|---|---|---|
| Health Canada (HC) | 2019 | $114,388.00 |
| Health Canada (HC) | 2020 | $150,681.00 |
| Public Health Agency of Canada (PHAC) | 2017 | $687,500.00 |
| Public Health Agency of Canada (PHAC) | 2018 | $121,142.00 |
| Public Health Agency of Canada (PHAC) | 2019 | $633,191.50 |
| Public Health Agency of Canada (PHAC) | 2020 | $664,891.00 |
| Public Health Agency of Canada (PHAC) | 2021 | $120,824.00 |
| Public Health Agency of Canada (PHAC) | 2021 | $1,802,583.00 |
| Public Services and Procurement Canada (PSPC) | 2019 | $2,411,120.76 |
| Public Services and Procurement Canada (PSPC) | 2020 | $2,689,025.00 |
What a shocker. The Public Health Agency of Canada (PHAC), and Health Canada, are both major contributors to the Canadian Paediatric Society. Interestingly, those are dwarfed in size by Public Services and Procurement Canada.
One of the lobbyists, Samantha Grill, used to work for the Aga Khan Foundation, but that probably has no connection with anything. Most likely it’s just a coincidence.
The recent grants from Procurement Canada appear to come as part of contracts to engage in tracking and surveillance of health issues in Canada. In other words, The CPS is effectively hired to collect research data on young children as part of Canada’s policy formations.
The above information is available from the Lobbying Registry, and Open Search, two Government-run databases which track grants to various organizations.
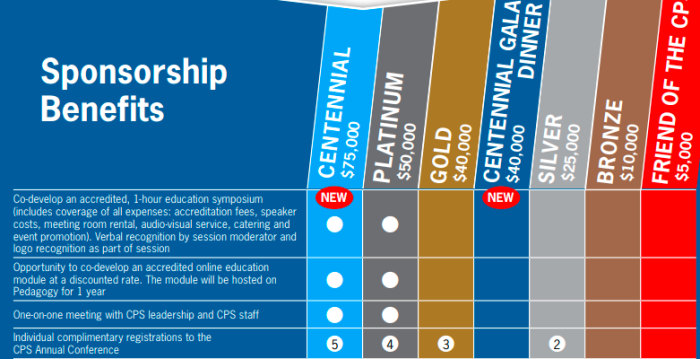
To address the elephant in the room: does the CPS take private money? Yes it does, in the form of sponsorships. For the low price of $50,000 or $75,000 one can receive the following additional benefits:
- Co-develop an accredited, 1-hour education symposium (includes coverage of all expenses: accreditation fees, speaker costs, meeting room rental, audio-visual service, catering and event promotion). Verbal recognition by session moderator and logo recognition as part of session
- Opportunity to co-develop an accredited online education module at a discounted rate. The module will be hosted on. Pedagogy for 1 year
- One-on-one meeting with CPS leadership and CPS staff
This was outlined in a paper promoting the conference in May 2022. Now, who would want to develop education modules, or education symposiums? Why, drug companies of course. That way, paediatricians can be “educated” in the latest wonder drug that big pharma has to offer.
It seems unlikely that individuals would be interested in dropping this kind of money, regardless of the prestige. However, a drug company would just see this as the cost of doing business.
This comes across as a pay-to-play system where a large enough cheque means determining what gets addressed with other members.
Of course, this issue isn’t limited to the Canadian group. The Provinces also have similar organizations, and they also appear to be compromised. Take the time to do your own research.
(1) https://cps.ca/
(2) https://caringforkids.cps.ca/handouts/healthy-living/masks-and-children-during-covid
(3) https://cps.ca/en/about-apropos
(4) https://cps.ca/documents/position/clinical-guidance-for-youth-with-myocarditis-and-pericarditis
(5) Canadian Paediatric Society Pericarditis Myocarditis
(6) http://web.archive.org/web/20211220062530/https://cps.ca/en/documents/position/vaccine-for-children-5-to-11
(7) https://apps.cra-arc.gc.ca/ebci/hacc/srch/pub/dsplyRprtngPrd?q.srchNmFltr=paediatric&q.stts=0007&selectedCharityBn=118920412RR0001&dsrdPg=1
(8) Canadian Paediatric Foundation Charity
(9) https://search.open.canada.ca/en/gc/
(10) https://lobbycanada.gc.ca/app/secure/ocl/lrs/do/vwRg?cno=258842®Id=918505
(11) https://buyandsell.gc.ca/procurement-data/tender-notice/PW-SS-041-34649
(12) https://twitter.com/CanPaedSociety
(13) https://cps.ca/uploads/about/Final_-_2022_CPS_Sponsorship_Opportunities_Document_-_August_20_-_2021.pdf
(14) Final_-2022_CPS_Sponsorship_Opportunities_Document–August_20-_2021
(15) https://www.linkedin.com/in/samantha-grills-ba240742/details/experience/
(16) Experience _ Samantha Grills _ LinkedIn
(A) https://canucklaw.ca/health-canada-initially-created-for-population-control-measures/
(B) https://canucklaw.ca/cv-62g-public-health-agency-of-canada-created-as-branch-of-who
(C) https://canucklaw.ca/canadian-pharmaceutical-sciences-foundation-a-registered-charity-funded-by-drug-companies/
(D) https://canucklaw.ca/canadian-pharmacists-association-campaigning-at-taxpayer-expense-to-grow-big-drug-industry/
(E) https://canucklaw.ca/canadian-immunization-research-network-is-funded-by-big-pharma/
(F) https://canucklaw.ca/society-of-obstetricians-and-gynaecologists-funded-by-pfizer-recommends-vaccines-boosters/
(G) https://canucklaw.ca/canimmunize-working-with-big-pharma-on-national-vaccination-certification-medical-research/