
Even as the world crumbles due to a fake pandemic, clowns like B.C. Premier John Horgan, and B.C. Provincial Health Officer Bonnie Henry think it’s all fun and games. They push degeneracy and filth while stripping residents of their rights.
This piece is designed to lay out, in plain terms, the lack of any real science behind this “pandemic”. Despite what all the experts are saying, it’s pretty baseless. Before getting into the heart of the article, let’s address 3 points:
First: Canada really has no sovereignty in the matter. This is something our politicians know, but seem content with otherwise. As part of our membership with the World Health Organization, we must follow the IHR, or International Health Regulations. The latest is from 3rd Edition, in 2005. WHO’s Constitution (specifically Articles 21(A) and 22) are clear on quarantine measures. On a related note, the 2005 Quarantine Act was based on the IHR. See this transcript from November 4, 2004.
Second: M-132 is a Motion introduced in 2017 by a connected pharmacist for Canada to finance drugs and drug research in Canada — and abroad. That’s correct, this was brought into the House of Commons over 2 years BEFORE this outbreak.
Motion Text
That the Standing Committee on Health be instructed to undertake a study on ways of increasing benefits to the public resulting from federally funded health research, with the goals of lowering drugs costs and increasing access to medicines, both in Canada and globally; and that the Committee report its findings and recommendations to the House no later than one year from the time this motion is adopted.
Third: the full scale of the pharmaceutical lobbying is something unknown to most people. Trudeau, O’Toole, Ford, Pallister, Kenney and Horgan are all compromised. They cannot be trusted to act in Canada’s best interest. It cannot be understated how much money there is, not just in vaccines, but in testing kits, and other pandemic related expenses. It doesn’t help that our media and fact-checkers are also co-opted.
Now, let’s get into the lack of real science. These are the topics to be addressed.
#1: Virus has never been isolated
#2: Virus isolation not used for diagnostics
#3: Being infectious is completely subjective
#4: Re-Testing is frequently advised
#5: Models are not evidence of anything
#6: RT-PCR test not designed for infection detection
#7: Error rate in RT-PCR tests is unknown
#8: Antibody tests very unreliable
#9: Deceit in reporting death count
#10: No basis for 2m “social distancing”
#11: No solid evidence masks actually work
#12: No science behind group size limits
#13: No science behind selective business closures
#14: No science behind curfew/house arrest
#15: Borders are kept open during “pandemic”
#16: Limited testing with mRNA “Vaccines”
#17: Changing definition of “herd immunity”
#18: Bonnie Henry’s deception on masks/vaccines
#19: Psychological research into getting people vaccinated
This list is not exhaustive, but should provide some insight into just how meaningless many of these scientific claims are. There’s no foundation for them. Going through them individually:
[1] Virus Has Never Been Isolated
This was addressed in depth by Christine Massey of Fluoride Feel Peel. The short version is that Governments CLAIM they have isolated this virus, and all subsequent actions are based on science. Problem is: every one so far who has been served with a freedom-of-information request has either stalled, or reported back that no records were found.
A little experiment was done here to try to replicate FFP’s work. While most FOIs are still outstanding, some, including the Canadian Institute for Health Research and the National Research Council confirmed they have no records.
[2] Virus Not Isolated For Diagnostics
[March 2020, Page 3]
Viral culture
Virus isolation is not recommended as a routine diagnostic procedure.
[September 2020, Page 8]
Viral isolation
Virus isolation is not recommended as a routine diagnostic procedure. All procedures involving viral isolation in cell culture require trained staff and BSL-3 facilities. A thorough risk assessment should be carried out when culturing specimens from potential SARSCoV-2 patients for other respiratory viruses because SARS-CoV-2 has been shown to grow on a variety of cell lines [183].
[Health Canada, April 2, 2020]
Confirmed
A person with laboratory confirmation of infection with the virus that causes COVID-19 performed at a community, hospital or reference laboratory (NML or a provincial public health laboratory) running a validated assay. This consists of detection of at least one specific gene target by a NAAT assay (e.g. real-time PCR or nucleic acid sequencing).
[BC CDC Guidelines]
Confirmed case
A person with laboratory confirmation of infection with the virus that causes COVID-19 performed at a community, hospital or reference laboratory (NML or a provincial public health laboratory) running a validated assay. This consists of detection of at least one specific gene target by a NAAT assay (e.g. real-time PCR or nucleic acid sequencing).
[Alberta Public Health, Page 3]
Confirmed Case
A person with laboratory confirmation of infection with the virus (SARS-CoV-2) that causes
COVID-19 which consists of:
• Detection of at least one specific gene target by nucleic acid amplification tests (NAAT) at
a Provincial Public Health Laboratory where NAAT tests have been validated(A)
;
OR
• Confirmed positive result by National Microbiology Lab (NML) by NAAT.
[Manitoba Guidance]
Confirmed case – A person with a laboratory confirmation of infection with the virus that causes COVID-19 performed at a community, hospital or reference laboratory (NML or a provincial public health laboratory) running a validated assay. This consists of detection of at least one specific gene target by a NAAT assay (e.g. real-time PCR or nucleic acid sequencing).
[Ontario Public Health]
Specimens tested using the in-house laboratory developed assay will be tested using the E gene real-time PCR assay, the more sensitive of the two PCR targets.
.
-Specimens with a single target detected (regardless of assay used) will be reported as COVID-19 virus detected, which is sufficient for laboratory confirmation of COVID-19 infection.
-Specimens with no gene target(s) detected in the assay used will be reported as COVID-19 virus not detected.
WHO’s information from March 19, 2020, and September 11 both recommend AGAINST isolating the virus for the purpose of diagnosing a patient. Health Canada, the BC CDC, Alberta Public Health, Manitoba Health, and Ontario Public Health all say that detection of a single gene is sufficient. No virus isolation is needed.
[3] Being Infectious Is Completely Subjective
[March 20, Page 1]
Case definitions for surveillance
Case and contact definitions are based on the current available information and are regularly revised as new information accumulates. Countries may need to adapt case definitions depending on their local epidemiological situation and other factors. All countries are encouraged to publish definitions used online and in regular situation reports, and to document periodic updates to definitions which may affect the interpretation of surveillance data.
In their March 20, 2020 guidance, WHO actually suggested countries come up with their own standards and definitions of what a “case” was.
[4] Re-Testing Is Frequently Advised
[January 17, Page 1]
3. Specimen collection and shipment Rapid collection and testing of appropriate specimens from suspected cases is a priority and should be guided by a laboratory expert. As extensive testing is still needed to confirm the 2019-nCoV and the role of mixed infection has not been verified, multiple tests may need to be performed and sampling sufficient clinical material is recommended. Local guidelines should be followed regarding patient or guardian’s informed consent for specimen collection, testing and potentially future research.
[March 19, Page 2]
One or more negative results do not rule out the possibility of COVID-19 virus infection. A number of factors could lead to a negative result in an infected individual, including:
poor quality of the specimen, containing little patient material (as a control, consider determining whether there is adequate human DNA in the sample
by including a human target in the PCR testing).
the specimen was collected late or very early in the infection.
the specimen was not handled and shipped appropriately.
technical reasons inherent in the test, e.g. virus mutation or PCR inhibition.
[March 19, Page 3]
If a negative result is obtained from a patient with a high index of suspicion for COVID-19 virus infection, particularly when only upper respiratory tract specimens were collected, additional specimens, including from the lower respiratory tract if possible, should be collected and tested.
[September 11, Page 6]
Careful interpretation of weak positive NAAT results is needed, as some of the assays have shown to produce false signals at high Ct values. When test results turn out to be invalid or questionable, the patient should be resampled and retested. If additional samples from the patient are not available, RNA should be re-extracted from the original samples and retested by highly experienced staff. Results can be confirmed by an alternative NAAT test or via virus sequencing if the viral load is sufficiently high. Laboratories are urged to seek reference laboratory confirmation of any unexpected results
[September 11, Page 7]
Rapid diagnostic tests that detect the presence of SARS-CoV-2 viral proteins (antigens) in respiratory tract specimens are being developed and commercialized. Most of these are lateral flow immunoassays (LFI), which are typically completed within 30 minutes. In contrast to NAATs, there is no amplification of the target that is detected, making antigen tests less sensitive. Additionally, false positive (indicating that a person is infected when they are not) results may occur if the antibodies on the test strip also recognize antigens of viruses other than SARS-CoV-2, such other human coronaviruses.
[January 13, 2021]
WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology.
WHO’s own guidance from January 17, 2020, and March 19, 2020, September 11, 2020, and January 13, 2021, (archived), indicate that people should be retested if there was suspicion. That doesn’t exactly scream out that the test is reliable.
[5] Models Are Predictions, Not Evidence
WHO’s dictates are based on modelling. In June 2020, they thought that 6% to 41% of the global population was infected. In other words, they have no idea.
This needs to be addressed head on: models are not evidence of anything. Instead, they are projections, predictions of what people BELIEVE will happen. It’s entirely possible that the people running them have their own political agendas. But even sincere people are limited by their own data and understanding of what they are doing.
As for these outfits being compromised, consider these 3, all of whom have financial ties to the Bill & Melinda Gates Foundation:
- Imperial College London
- London School of Hygiene & Tropical Medicine
- Vaccine Impact Modelling Consortium
Whenever a politician or “expert” talks about their modelling predicting something, it is not evidence. It is pseudo-science, being used to push a narrative.
[6] RT-PCR Tests Never Designed For This
[Australia, April 3, Page 1/2]
Can reinfection occur?
There have been reports of apparent re-infection in a small number of cases. However, most of these describe patients having tested positive within 7-14 days after apparent recovery. Immunological studies indicate that patients recovering from COVID-19 mount a strong antibody response. It is likely that positive tests soon after recovery represent persisting excretion of viral RNA, and it should be noted that PCR tests cannot distinguish between “live” virus and noninfective RNA. Australian guidelines currently require patients who have had COVID-19 to test negative on two tests 24 hours apart before being released from isolation.
COVID-19 testing in Australia – information for health professionals
1 October 2020
Tests for COVID-19 aim to detect the causative virus, SARS-CoV-2, or an immune response to SARS-CoV-2. The reliability of COVID-19 tests is uncertain due to the limited evidence base. Available evidence mainly comes from symptomatic patients, and their clinical role in detecting asymptomatic carriers is unclear.
.
The indications for conducting a COVID-19 test have changed through the course of the pandemic. See the current suspect case definition (link is external) and the testing criteria (link is external) on the Department of Health website.
[Australia, October 8]
Nucleic acid tests
These tests detect the presence of the genetic material, called nucleic acids, of the actual SARS-CoV-2 virus. Such tests are good at detecting the virus early in the infection and can sometimes even detect the virus in a person before they become unwell. There are several types of nucleic acid tests that can be used to detect the SARS-CoV-2 virus, including polymerase chain reaction (PCR) tests and isothermal nucleic acid amplification tests (e.g., loop-mediated isothermal amplification (LAMP) tests).
.
PCR tests are generally considered better at detecting the presence of the SARS-CoV-2 virus and are currently the gold standard for diagnosis of COVID-19.
The Australian Department of Health released information on April 3 about this virus, but admitted that PCR tests cannot distinguish between “live” and “noninfective” RNA. In other words, it’s pretty useless. Even on October 1, this archived page stated that the limited evidence made the test unreliable.
But what a difference a week makes. In this October 8 posting, PCR tests are now the gold standard. In April, they couldn’t tell between dead and live genetic material. October 1, the reliability was uncertain. Now, it’s the gold standard.
Just consider the creator of the test, Kary Mullis. He has publicly said that RT-PCR was never designed to test for infection, and hence is meaningless, from a scientific perspective.
[7] Error Rate In RT-PCR Tests Unknown
[BC CDC April, 30]
1. How does the test work?
The NAT works by detecting RNA specific to the SARS-CoV-2 virus that causes COVID-19 infection, after RNA has been extracted from the specimen and then amplified in the laboratory. NATs are typically performed on nasopharyngeal swabs, but the test can also be done on other sample types such as throat swabs, saliva, sputum, tracheal aspirates, and broncho-alveolar lavage (BAL) specimens.
.
The NAT has a high analytical sensitivity (i.e., it works well at detecting the virus when the virus is present). The NAT can potentially detect as few as 10-100 copies of viral RNA per mL in a respiratory sample. Note that this is not the same as clinical sensitivity of NAT for detection of COVID-19 infection, which is unknown at this time (see #5 below).
[BC CDC, April 30]
2. What do the test results mean?
Positive: Viral RNA is detected by NAT and this means that the patient is confirmed to have COVID-19 infection.
A positive NAT does not necessarily mean that a patient is infectious, as viral RNA can be shed in the respiratory tract for weeks but cultivatable (live) virus is typically not detected beyond 8 to 10 days after symptom onset.
Negative: Viral RNA is not detected in the sample. However, a negative test result does not totally rule out COVID-19 infection as there may be reasons beyond test performance that can result in a lack of RNA detection in patients with COVID-19 infection (false negatives; see below).
Indeterminate: The NAT result is outside the validated range of the test (i.e., RNA concentration is below the
limit of detection, or a non-specific reaction), or this might occur when the sample collected is of poor quality
(i.e., does not contain a sufficient amount of human cells). Indeterminate results do not rule in or rule out infection.
[BC CDC April 30]
5. What is the clinical sensitivity of the NAT test?
A statistic commonly quoted is that there is a 30% chance of a false negative result for a NAT test in a patient with COVID-19 infection (i.e., a 70% sensitivity). These and other similar estimates are based on a small number studies that compared the correlation between CT scan findings suggestive of COVID-19 infection to NAT on upper respiratory tract specimens. In these studies, 20-30% of people with a positive CT scan result had negative NAT results – and as discussed above a number of factors can contribute to false negative results. CT scan is not a gold standard for diagnosis ofCOVID-19 infection, and CT scan cannot differentiate amongst the many microbiological causes of pneumonia.
.
Ultimately, for COVID-19 testing, there is currently no gold standard, and the overall clinical sensitivity and specificity of NAT in patients with COVID-19 infection is unknown (i.e., how well NAT results correlate with clinical infection, “true positivity” or “true negativity” rate).
[Alberta Health Services, April 30]
The analytical validity of the lab-developed test used in Alberta is not in question, as confirmatory testing by the Canadian National Microbiology Lab (NML) showed that the Alberta test was 100% accurate, and analytical specificity of PCR testing has been reported to be 100% given the methodology – at least when done during active infection phase.
The videos are of Barbara Yaffe, the Deputy Medical Officer of Ontario, and Jason Kenney, the Premier of Alberta. Yaffe admits that there can be 50% errors with RT-PCR tests, and Kenney seems indifferent that it could be 90%.
What this means is that the BC CDC admits that it has no idea about the reliability of the tests. Positive or negative tests could be wrong
Alberta Health Services claims the test is 100% effective (page 1), but with the HUGE disclaimer that it applies during active infection. That could mean an avalanche of false positives.
[8] Antibody Tests Very Unreliable
[Sask Health Authority, Page 4]
Provides preliminary test results:
Negative: Does NOT rule out COVID-19 infection. Does NOT change any infection control precautions or isolation requirements.
Positive: Should be acted on immediately. Considered a “Presumptive Case” until confirmed by an in-lab PCR test.
Confirmatory Testing must be performed on:
• All Positives
• Unresolved Invalid tests and
• Negatives where patient is suspected of COVID-19infection.
A new NP swab should be collected, placed in viral transport media, and referred to a SHA Laboratory for confirmatory testing.
BC Provincial Health Officer, Bonnie Henry, admits that anitbody tests are of limited use and effect. Henry also admits the “false positivity rate” and the “false negative rate” can be very high. According to the Saskatchewan Health Authority, antigen tests, at least this particular one, provide preliminary results, and nearly always have to be followed up. That doesn’t exactly come across as reliable, not that the PCR test is any better.
[9] Outright Deceit Concerning Death Counts
[WHO, April 16, 2020, Page 3]
1. PURPOSE OF THE DOCUMENT
This document describes certification and classification (coding) of deaths related to COVID-19. The primary goal is to identify all deaths due to COVID-19.
.
A simplified section specifically addresses the persons that fill in the medical certificate of cause of death. It should be distributed to certifiers separate from the coding instructions.
[WHO, April 16, 2020, Page 3]
2. DEFINITION FOR DEATHS DUE TO COVID-19
A death due to COVID-19 is defined for surveillance purposes as a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma). There should be no period of complete recovery from COVID-19 between illness and death.
.
A death due to COVID-19 may not be attributed to another disease (e.g. cancer) and should be counted independently of preexisting conditions that are suspected of triggering a severe course of COVID-19.
[August 7, Page 3]
3. Definition of death due to COVID-19
A COVID-19 death is defined for surveillance purposes as a death resulting from a clinically compatible illness in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID-19 disease (e.g. trauma). There should be no period of complete recovery between the illness and death.
[December 16, Page 2]
Probable COVID-19 case:
A. A patient who meets clinical criteria above AND is a contact of a probable or confirmed case, or epidemiologically linked to a cluster of cases which has had at least one confirmed case identified within that cluster.
B. A suspected case (described above) with chest imaging showing findings suggestive of COVID-19 disease*
* Typical chest imaging findings suggestive of COVID-19 include the following (Manna 2020):
• chest radiography: hazy opacities, often rounded in morphology, with peripheral and lower lung distribution
• chest CT: multiple bilateral ground glass opacities, often rounded in morphology, with peripheral and lower lung
distribution
• lung ultrasound: thickened pleural lines, B lines (multifocal, discrete, or confluent), consolidative patterns with or without air bronchograms.
C. A person with recent onset of anosmia (loss of smell) or ageusia (loss of taste) in the absence of any other identified cause.
D. Death, not otherwise explained, in an adult with respiratory distress preceding death AND who was a contact of a probable or confirmed case or epidemiologically linked to a cluster which has had at least one confirmed case identified within that cluster.
[December 16, Page 3]
3. Definition of death due to COVID-19
A COVID-19 death is defined for surveillance purposes as a death resulting from a clinically compatible illness in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID-19 disease (e.g. trauma). There should be no period of complete recovery between the illness and death.
According to WHO’s April 16, and August 7 2020 guidelines, a person dying of a “clinical compatible illness” is sufficient to label as a “Covid death”. That standard is also repeated in the instructions as recently as December 16, 2020.
It would be nice to just blame this on some dishonest politicians, like Ontario Health Minister Christine Elliott, but the problem goes much deeper than that. It’s a coordinated effort to deceive the public into what’s happening.
[10] No Basis For 2 Metre “Social Distancing”
About this so called “social distancing”, where are the lengths determined? 2 metres and 6 feet are not equivalent, but even so, where did that come from? There are many references on WHO’s site to 1 METRE but nothing above that. Is it made up as well?
[11] No Real Evidence Masks Work At All
WHO released their “interim guidance” on April 6, June 5 and December 1, 2020. There was another release August 21 that specifically addressed children and masks.
What’s very telling is they are very wishy-washy in all reports. Many times it’s stated that either there’s no real evidence, or that more study is needed. Even taking a very charitable interpretation, the support for masks (based on science), is lukewarm.
However, based on the claims routinely touted in the media, one would think this is a settled issue, and that there’s no room for debate. Even the BBC knows this is political.
[12] No Science Behind Group Size Limits
Canadians have the right to freely associate, and to peacefully assemble. If Governments are going to infringe on that, there has to be a valid reason. They have yet to demonstrate one.
Beyond that, why is it that groups of 10 are allowed in Ontario, but groups of 50 are fine in B.C.? What is the scientific rational for these cut-offs? As it turns out, there is no real science behind any of it, as Bonnie Henry repeatedly jokes. Apparently as long as it’s “consistent”, being baseless is irrelevant.
The first video came from the Vancouver Sun. See the 1:00 mark. The second is from TCN TV.
[13] No Science Behind Business Closures
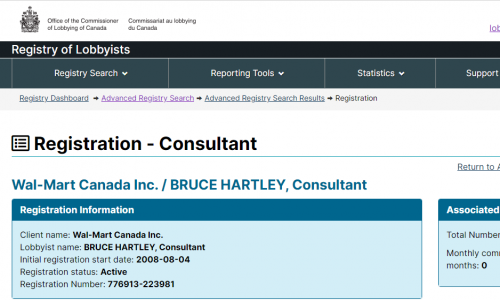
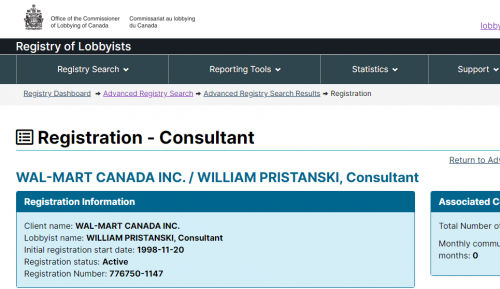
Throughout this so-called “pandemic”, rules around business closures have been applied unevenly, and in an arbitrary manner. Shutting down businesses and destroying people’s livelihoods is wrong to begin with, but why all of the double standards? It could be because places like Walmart have been lobbying politicians in Canada. This is about political connections, not science.
Who are Bruce Hartley and William Pristanski? Those are the same lobbyists who got SNC Lavalin their deferred prosecution agreement. Very well connected.
[14] No Science With Curfews/House Arrest
This ties back to the modelling addressed earlier. Ford, Legault, and others have claimed that people need to be home during certain hours, as the computer models say this will cut the number of cases. Okay, what is any of this based on? This is nothing more than martial law cloaked as public health.
[15] Keeping Borders Open During “Pandemic”


[January 2020 IHR guidelines]
The Committee does not recommend any travel or trade restriction based on the current information available.
[May 2020 IHR guidelines]
The WHO Regional Emergency Directors and the Executive Director of the WHO Health Emergencies Programme (WHE) provided regional and the global situation overview. After ensuing discussion, the Committee unanimously agreed that the outbreak still constitutes a public health emergency of international concern (PHEIC) and offered advice to the Director-General.
Travel and Trade
Continue working with countries and partners to enable essential travel needed for pandemic response, humanitarian relief, repatriation, and cargo operations.
.
Develop strategic guidance with partners for the gradual return to normal operations of passenger travel in a coordinated manner that provides appropriate protection when physical distancing is not feasible.
[August IHR guidelines]
(8) Work with partners to revise WHO’s travel health guidance to reinforce evidence-informed measures consistent with the provisions of the IHR (2005) to avoid unnecessary interference with international travel; proactively and regularly share information on travel measures to support State Parties’ decision-making for resuming international travel.
Throughout 2020, the WHO didn’t recommend any travel restrictions, despite this “supposedly” being a deadly outbreak. Their January, May and August releases made that clear. This isn’t to defend Trudeau, but he was just following the orders of his masters. So politicians pretending to be outraged are lying to the cameras.
Not only are there real travel restrictions, immigration has not suffered any cuts. In fact, there are efforts to greatly increase it. CANZUK, (the open borders scheme with Canada, Australia, New Zealand and the U.K.), is apparently still underway.
Illegal crossings (Lacolle at Roxham Road), haven’t stopped either. In fact, it has been converted into a LEGAL pprt of entry.
[16] Limited Testing With mRNA “Vaccines”

Moderna and Pfizer have had their “vaccines” approved by Health Canada. Of course, given what they actually are, it may be more accurate to refer to them as a form of gene replacement therapy.
Nonetheless all political parties seem content with letting this go ahead, in spite of the testing issues listed in their inserts.
[Section 30.1 of Food & Drug Act]
“The Minister may make an interim order that contains any provision that may be contained in a regulation made under this Act if the Minister believes that immediate action is required to deal with a significant risk, direct or indirect, to health, safety or the environment.”
What Section 30.1 means is that the Health Minister is allowed to sign an Order allowing vaccines to be distributed in Canada, even if they haven’t fully tested it.
[17] Changing Definition Of “Herd Immunity”
What is herd immunity?
Herd immunity is the indirect protection from an infectious disease that happens when a population is immune either through vaccination or immunity developed through previous infection. This means that even people who haven’t been infected, or in whom an infection hasn’t triggered an immune response, they are protected because people around them who are immune can act as buffers between them and an infected person. The threshold for establishing herd immunity for COVID-19 is not yet clear.
‘Herd immunity’, also known as ‘population immunity’, is a concept used for vaccination, in which a population can be protected from a certain virus if a threshold of vaccination is reached.
.
Herd immunity is achieved by protecting people from a virus, not by exposing them to it. Read the Director-General’s 12 October media briefing speech for more detail.
.
Vaccines train our immune systems to develop antibodies, just as might happen when we are exposed to a disease but – crucially – vaccines work without making us sick. Vaccinated people are protected from getting the disease in question. Visit our webpage on COVID-19 and vaccines for more detail.
.
As more people in a community get vaccinated, fewer people remain vulnerable, and there is less possibility for passing the pathogen on from person to person. Lowering the possibility for a pathogen to circulate in the community protects those who cannot be vaccinated due to other serious health conditions from the disease targeted by the vaccine. This is called ‘herd immunity’.
October 22, 2020 definition, the November 5 definition (which edits out previous infection), and what the site says on December 31. A possible explanation is that WHO’s edits were publicly called out, so they reverted back to the original definition.
[18] Bonnie Henry Lies About Masks/Vaccinations
134. Dr. Henry agreed with this observation by Dr. Skowronski and Dr. Patrick who are her colleagues at the British Columbia Centre for Disease Control:
.
I do agree, as we’ve discussed earlier, influenza is mostly transmitted in the community and we don’t have data on the difference between vaccinated and unvaccinated healthcare workers and individual transmission events…in healthcare settings.
.
135. Dr. Henry agreed that no VOM policy would influence influenza in the community. Dr. McGeer denied that she had used or recommended the use of community burden in the assessment of development of such a policy.
160. In direct examination Dr. Henry stated that the pre-symptomatic period was “clearly not the most infectious period but we do know that it happens”.[203] She also agreed in cross-examination that transmission required an element of proximity and a sufficient amount of live replicating virus.
.
161. At another point, the following series of questions and answers ensued during Dr. Henry’s cross-examination:
.
Q. With respect to transmission while asymptomatic, and I want to deal with your authorities with respect to that, would you agree with me that there is scant evidence to support that virus shedding of influenza actually leads to effective transmission of the disease before somebody becomes symptomatic?
.
A. I think we talked about that yesterday, that there is some evidence that people shed prior to being symptomatic, and there is some evidence of transmission, that leading to transmission, but I absolutely agree that that is not the highest time when shedding and transmission can occur.
.
Q. So were you—I put it to you that there’s scant evidence, and that was Dr. De Serres’ evidence, so—but that there’s very little evidence about that, do you agree?
.
A. There is—as we talked about yesterday, there is not a lot of evidence around these pieces, I agree.
.
Q. And clearly transmission risk is greatest when you’re symptomatic, when you’re able to cough or sneeze?
.
A. Transmission risk is greatest, as we’ve said, when you’re symptomatic, especially in the first day or two of symptom onset
177. Dr. McGeer and Dr. Henry presented the position of the OHA and the Hospital based upon their understanding of the relevant literature. Neither of them asserted that they had particular expertise with respect to masks or had conducted studies testing masks.
184. In her pre-hearing Report Dr. Henry responded to a request that she discuss the evidence that masks protect patients from influenza this way:
.
There is good evidence that surgical masks reduce the concentration of influenza virus expelled into the ambient air (a 3.4 fold overall reduction in a recent study) when they are worn by someone shedding influenza virus. There is also evidence that surgical masks reduce exposure to influenza in experimental conditions.
.
Clinical studies have also suggested that masks, in association with hand hygiene, may have some impact on decreasing transmission of influenza infection. These studies are not definitive as they all had limitations. The household studies are limited by the fact that mask wearing did not start until influenza had been diagnosed and the patient/household was enrolled in the study, such that influenza may have been transmitted prior to enrollment. A study in student residences is limited by the fact that participants wore their mask for only approximately 5 hours per day. Two systematic reviews of the cumulative studies conclude that there is evidence to support that wearing of masks or respirators during illness protects others, and a very limited amount of data to support the use of masks or respirators to prevent becoming infected
.
In summary, there is evidence supporting the use of wearing of masks to reduce transmission of influenza from health care workers to patients. It is not conclusive, and not of the quality of evidence that supports influenza vaccination. Based on current evidence, patient safety would be best ensured by requiring healthcare providers to be vaccinated if they provide care during periods of influenza activity. However, if healthcare workers are unvaccinated, wearing masks almost certainly provides some degree of protection to their patients.
219. Dr. Henry answered the ‘why not mask everyone’ question this way:
.
It is [influenza vaccination] by far, not perfect and it needs to be improved, but it reduces our risk from a hundred percent where we have no protection to somewhat lower. And there’s nothing that I’ve found that shows there’s an incremental benefit of adding a mask to that reduced risk…..there’s no data that shows me that if we do our best to reduce that incremental risk, the risk of influenza, that adding a mask to that will provide any benefit. But if we don’t have any protection then there might be some benefit when we know our risk is greater.
.
When we look at individual strains circulating and what’s happening, I think we need it to be consistent with the fact that there was nothing that gave us support that providing a mask to everybody all the time was going to give us any additional benefit over putting in place the other measures that we have for the policy. It’s a tough one. You know, it varies by season.[320]
.
It is a challenging issue and we’ve wrestled with it. I’m not a huge fan of the masking piece. I think it was felt to be a reasonable alternative where there was a need to do—to feel that we were doing the best we can to try and reduce risk.
.
I tried to be quite clear in my report that the evidence to support masking is not as great and it is certainly not as good a measure
Bonnie Henry testified as an expert witness in a 2015 case, Ontario Nurses Association v.s. Sault Area Hospital. She testified there was little evidence that the hospital’s “vaccinate or mask” policy worked rearding influenza. At best, she really seemed to be hedging her answers, and avoiding direct conclusions.
Now she says something quite different in 2020.
[19] Psyche Research Into “Vaccine Hesitancy”

It would be remiss to claim there is no science at all, without mentioning the science that “does” take place. Specifically, plenty of psychological and sociological research is done into convincing people that vaccines are safe, and necessary.
To clarify, this research is not about ENSURING that the vaccines people get are safe. Instead, it is research into CONVINCING people that they already are. Big difference.
Part 1: Canada’s vaccine strategy, tax-funded programs
Part 2: The Vaccine Confidence Project
Part 3: More research into “Vaccine Hesitancy”
Part 4: Psychological manipulaton
Part 5: WEF meeting to discuss boosting vaccination levels
The above posts are from the website, and provide a decent introduction into this vast sub-area of research. Take the plunge for yourself
What Does All This Mean For Us?
For starters, it could mean the end of our free speech, if people like this have their way.
It’s difficult to believe that the public actually takes this “pandemic” seriously. However, that is the result when all of the information a person receives is controlled and manipulated.
Of course, we haven’t even gotten into the whole GREAT RESET. That is a plan by overlords to impose a New World Order in the face of this outbreak. Makes one seriously wonder if the whole thing was premeditated.
This is likely the most thorough and information packed blog I have ever followed!!
Thank you and don’t stop! You’re my encyclopedia.
Thanks for the dedicating your time and energy into creating such a valuable resource. (This research will be saved/shared/studied/discussed as a definitive expose on the fraud perpetrated on humanity.) Perhaps one day, those that orchestrated this horror will be held accountable. Nuremburg 2.0, perhaps?
The worrisome realization is that Nuremberg was put in place to prevent crimes against all of humanity and non-consenting human testing etc from happening again – yet it is has been repeated over and over and over.
I naively used to think only 3rd world Countries had criminal politicians that would perpetuate harm against their citizens – me being appalled with each revelation of harm and displacement outside of Canada.
And yet, here we are.
Probably one of the best websites about what’s truly going on in Canada…have been promoting it widely.