
Moving along, we get to New Brunswick, which is run by Blaine Higgs, who identifies as being a conservative. He has been in Office since November 2018, or about 3 years. So, he’s had some time to settle in.
Effective September 22, 2021, the Province had a vaccine passport in place. For a lack of a better term, these are “movement licenses” which allow people to maintain some semblance of freedom. (Credit to RoadtoSerfdom Twitter Account).
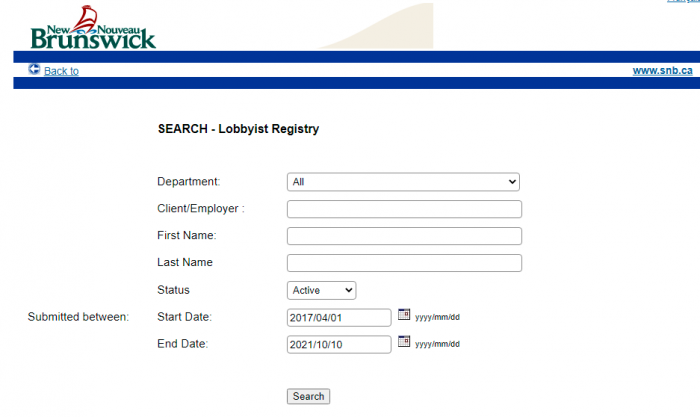
Let’s take a look at who Higgs has been talking to recently. Granted, some of the postings happened before he took power. Still, the same people keep coming around, trying to influence policy.
This series continues on who’s pulling the strings of influential politicians. Previously, Elizabeth May, Erin O’Toole, Michelle Rempel, Steven Guilbeault (Part 1 and Part 2), Doug Ford (many times), Rankin & Strang, Jason Kenney, Scott Moe and Brian Pallister were covered.

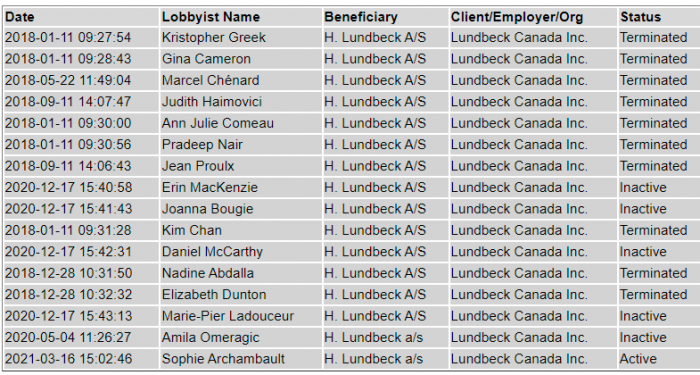



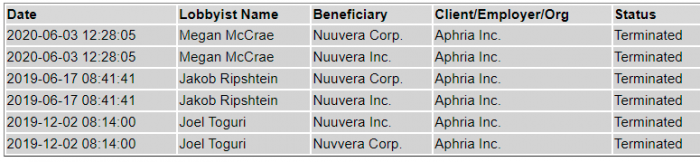

What a lot of pharma lobbying there has been in the last few years. And all this for a very small province. But don’t worry, because that certainly won’t impact how Higgs runs the affairs for New Brunswick.
1. Canadian Biosimilars Forum (Pfizer, Merck), Ross Wallace
Ross Wallace is part of Santis Health, which lobbied on behalf of Canadian Biosimilars Forum. The CSF is a coalition of pharma companies, much like Innovative Medicines Canada. Interestingly, Wallace worked for AstraZeneca for over 5 years prior to joining this group.
2. Innovative Medicines Canada, Pamela Fralick
Pamela Fralick and Innovative Medicines Canada were addressed in more detail earlier. IMC actually works as a collective to push for the joint interests of the pharmaceutical industry. See Item #4 for more information on them both
3. Innovative Medicines Canada, Cheryl Stewart-Walsh
Cheryl Stewart-Walsh is the Regional Director (Atlantic Canada) for Innovative Medicines Canada. Interestingly, she helped install Mike Savage as Mayor of Halifax, then worked in his office.
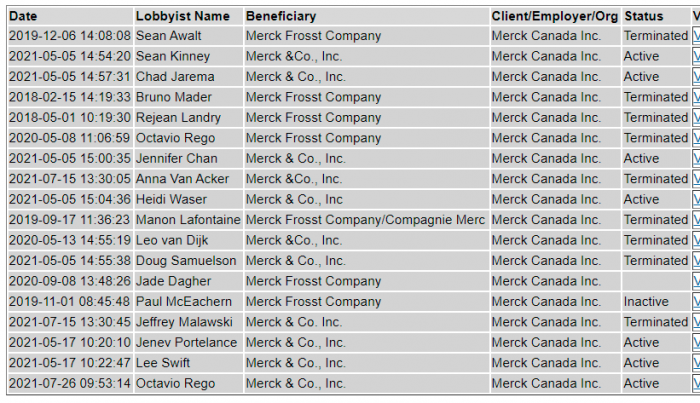
4. Merck Canada, Octavio Rego
Octavio Rego appears to have been in the pharma industry for the bulk of his working life. He spent 8 years at Sanofi, then another 13 at Merck.
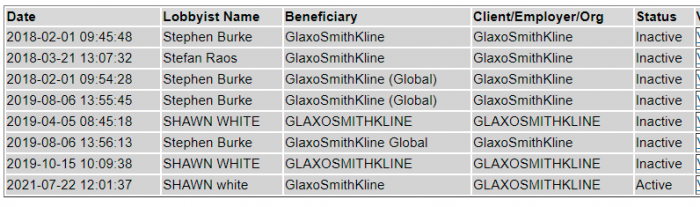
5. Purdue Pharma, Rémy Bouchard
Rémy Bouchard now works for Purdue, but has had a lengthy career in other companies. These include: Teva, AstraZeneca, and GlaxoSmithKline.
Side note: Higgs was part of the “coalition” of controlled opposition conservatives who pretended to oppose the Federal Carbon tax. Hard to challenge something when you enthusiastically support the overall agenda.
Anyhow, have a look around, and see what’s really happening. Want to know why all these politicians are so adamantly pro-vaxx? It’s not that complicated. Of course, this doesn’t take into account what may be happening off the books.
(1) https://www.youtube.com/watch?v=6qkTJMXYgok
(2) https://www.pxw1.snb.ca/snb9000/product.aspx?ProductID=A001PLOBBYSearch
(3) https://www.linkedin.com/in/ross-wallace-b6aa5948/
(4) https://www.canadianbiosimilarsforum.ca/
(5) https://www.linkedin.com/in/cheryl-stewart-walsh-785b3119/
(6) https://www.linkedin.com/in/r%C3%A9my-bouchard-6974a23/
(7) https://canucklaw.ca/whos-pulling-elizabeth-mays-strings/
(8) https://canucklaw.ca/whos-pulling-erin-otooles-strings/
(9) https://canucklaw.ca/why-is-rempel-silent-on-harmful-effects-of-interim-authorized-vaccines/
(10) https://canucklaw.ca/whos-pulling-steven-guilbeaults-strings-part-1-eco-movement/
(11) https://canucklaw.ca/whos-pulling-steven-guilbeaults-strings-part-2-anti-free-speech-privacy/
(12) https://canucklaw.ca/ford-still-lobbied-by-political-operatives-on-behalf-of-vaccine-companies/
(13) https://canucklaw.ca/cv-10d-nova-scotia-pharma-lobbying-moh-robert-strang-an-anti-democratic-tyrant/
(14) https://canucklaw.ca/whos-pulling-jason-kenneys-strings/
(15) https://canucklaw.ca/whos-pulling-scott-moes-strings/
(16) https://canucklaw.ca/whos-pulling-brian-pallisters-strings/