1. Other Articles On CV “Planned-emic”
This is a lengthy series, but a necessary read in order to understand what is really going on. This so-called pandemic is just a pretense for taking away more and more of your freedoms.
2. June 5, 2020 Interim Guidance
(Download the pdf at the bottom)
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/when-and-how-to-use-masks
WHO-2019-nCov-IPC_Masks-2020.4-eng (1)
(from page 4)
There are currently no studies that have evaluated the effectiveness and potential adverse effects of universal or targeted continuous mask use by health workers in preventing transmission of SARS-CoV-2. Despite the lack of evidence the great majority of the WHO COVID-19 IPC GDG members supports the practice of health workers and caregivers in clinical areas (irrespective of whether there are COVID-19 or other patients in the clinical areas) in geographic settings where there is known or suspected community transmission of COVID-19, to continuously wear a medical mask throughout their shift, apart from when eating and drinking or changing the mask after caring for a patient requiring droplet/contact precautions for other reasons (e.g., influenza), to avoid any possibility of cross-transmission
So there are no actual studies to test or research the effectiveness of masks in health care settings. However, it’s common practice to expect them to be worn.
(from page 6)
Available evidence
Studies of influenza, influenza-like illness, and human coronaviruses (not including COVID-19) provide evidence that the use of a medical mask can prevent the spread of infectious droplets from a symptomatic infected person (source control) to someone else and potential contamination of the environment by these droplets.(54, 55) There is limited evidence that wearing a medical mask by healthy individuals in households, in particular those who share a house with a sick person, or among attendees of mass gatherings may be beneficial as a measure preventing transmission.(41, 56-61) A recent meta-analysis of these observational studies, with the intrinsic biases of observational data, showed that either disposable surgical masks or reusable 12–16-layer cotton masks were associated with protection of healthy individuals within households and among contacts of cases.(42)
This could be considered to be indirect evidence for the use of masks (medical or other) by healthy individuals in the wider community; however, these studies suggest that such individuals would need to be in close proximity to an infected person in a household or at a mass gathering where physical distancing cannot be achieved, to become infected with the virus.
Results from cluster randomized controlled trials on the use of masks among young adults living in university residences in the United States of America indicate that face masks may reduce the rate of influenza-like illness, but showed no impact on risk of laboratory-confirmed influenza.(62, 63) At present, there is no direct evidence (from studies on COVID19 and in healthy people in the community) on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including COVID-19
The World Health Organization admits there is no direct evidence that widespread masking of healthy people actually prevents any sort of sickness. They speak on in terms of “indirect evidence” or being “possible”.
(from page 6)
2) Advice to decision makers on the use of masks for the
general public
.
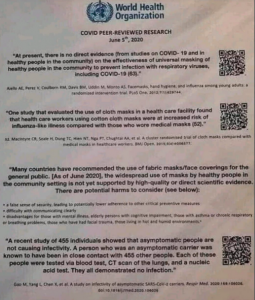
Many countries have recommended the use of fabric masks/face coverings for the general public. At the present time, the widespread use of masks by healthy people in the community setting is not yet supported by high quality or direct scientific evidence and there are potential benefits and harms to consider (see below).
However, taking into account the available studies evaluating pre- and asymptomatic transmission, a growing compendium of observational evidence on the use of masks by the general public in several countries, individual values and preferences, as well as the difficulty of physical distancing in many contexts, WHO has updated its guidance to advise that to prevent COVID-19 transmission effectively in areas of community transmission, governments should encourage the general public to wear masks in specific situations and settings as part of a comprehensive approach to suppress SARS-CoV-2 transmission (Table 2).
So no direct scientific evidence to support masking healthy people, but governments should encourage it anyway. Rather than focusing exclusively on science, it takes “values and preferences” into account. Perhaps this is why BCPHO Bonnie Henry says “there’s no science behind it”. It gets even better.
(from end of page 8/early 9)
A non-medical mask is neither a medical device nor personal protective equipment. However, a non-medical mask standard has been developed by the French Standardization Association (AFNOR Group) to define minimum performance in terms of filtration (minimum 70% solid particle filtration or droplet filtration) and breathability (maximum pressure difference of 0.6 mbar/cm2 or maximum Advice on the use of masks in the context of COVID-19: Interim guidance inhalation resistance of 2.4 mbar and maximum exhalation resistance of 3 mbar).
The lower filtration and breathability standardized requirements, and overall expected performance, indicate that the use of non-medical masks, made of woven fabrics such as cloth, and/or non-woven fabrics, should only be considered for source control (used by infected persons) in community settings and not for prevention. They can be used ad-hoc for specific activities (e.g., while on public transport when physical distancing cannot be maintained), and their use should always be accompanied by frequent hand hygiene and physical distancing.
So a non-medical mask isn’t actually considered PPE. But it’s nice to know that 70% is the new standard for being an acceptable filter. And despite them not being beneficial to healthy people, the World Health Organization recommends them anyway.
(from page 10)
WHO is collaborating with research and development partners and the scientific community engaged in textile
engineering and fabric design to facilitate a better understanding of the effectiveness and efficiency of nonmedical masks. WHO urges countries that have issued recommendations on the use of both medical and non-medical masks by healthy people in community settings to conduct research on this important topic. Such research needs to look at whether SARS-CoV-2 particles can be expelled through non-medical masks of poor quality worn by a person with symptoms of COVID-19 while that person is coughing, sneezing or speaking. Research is also needed on nonmedical mask use by children and other medically
challenging persons and settings as mentioned above.
World Health Organization recommends the use of masks, but admits that research needs to be done, and there’s no hard evidence that they work on healthy people.
3. April 6, 2020 Interim Guidance
https://apps.who.int/iris/handle/10665/331693
WHO-april-6-2019-nCov-IPC_Masks-2020
(page 1/2)
Medical masks should be reserved for health care workers. The use of medical masks in the community may create a false sense of security, with neglect of other essential measures, such as hand hygiene practices and physical distancing, and may lead to touching the face under the masks and under the eyes, result in unnecessary costs, and take symptoms. The true extent of asymptomatic infections will be determined from serologic studies. Advice on the use of masks in the context of COVID-19: interim guidance masks away from those in health care who need them most, especially when masks are in short supply.
(page 2)
Advice to decision makers on the use of masks for healthy people in community settings. As described above, the wide use of masks by healthy people in the community setting is not supported by current evidence and carries uncertainties and critical risks. WHO offers the following advice to decision makers so they apply a risk-based approach.
(page 2)
However, the following potential risks should be carefully
taken into account in any decision-making process:
• self-contamination that can occur by touching and
reusing contaminated mask
• depending on type of mask used, potential breathing
difficulties
• false sense of security, leading to potentially less
adherence to other preventive measures such as physical
distancing and hand hygiene
• diversion of mask supplies and consequent shortage of
mask for health care workers
• diversion of resources from effective public health
measures, such as hand hygiene
4. What Changed: April To June?


APRIL 2020: no evidence to support masking healthy people, and they need to be reserved for health care workers anyway.
JUNE 2020: no direct evidence to support masking healthy people, but governments should encourage it anyway.
Even taking the World Health Organization at face value (which is a stretch), they admit there is no hard evidence to support mandatory masking of healthy people. Governments are doing it of their own free will.