
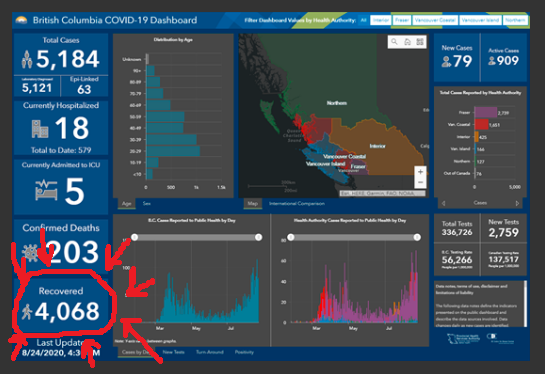
According to the BC Provincial Health Officer, the current tests can give up to 30% false negatives for people who are actually infected. Don’t worry, things are about to get a lot worse.
1. Other Articles On CV “Planned-emic”
The rest of the series is here. See the lies, lobbying, conflicts of interest, and various globalist agendas operating behind the scenes. There is a lot more than most people realize. For examples: The Gates Foundation finances many things, including, the World Health Organization, the Center for Disease Control, GAVI, ID2020, John Hopkins University, Imperial College London, the Pirbright Institute, and individual pharmaceutical companies.
2. Henry Admits “No Science” In 50-Person Limit

On May 25, 2020, BC Provincial Health Officer Bonnie Henry said that “50 cars” was included in the guidelines for limiting groups of people who can get together. At 1:05 she states that there is no real science behind these Provincial dictates. This was addressed in Part 37, but worth a review.
Also, it would be nice to get an explantion about the exemptions. The 50-person limit applies to movie theatres, but not grocery stores. It applies to religious gatherings, but not schools.
3. 2015 Testimony: Limited Evidence For Masks
https://www.canlii.org/en/on/onla/doc/2015/2015canlii62106/2015canlii62106.pdf
2015.ontario.college.of.nurses.mask.ruling
134. Dr. Henry agreed with this observation by Dr. Skowronski and Dr. Patrick who are her colleagues at the British Columbia Centre for Disease Control:
.
I do agree, as we’ve discussed earlier, influenza is mostly transmitted in the community and we don’t have data on the difference between vaccinated and unvaccinated healthcare workers and individual transmission events…in healthcare settings.
.
135. Dr. Henry agreed that no VOM policy would influence influenza in the community. Dr. McGeer denied that she had used or recommended the use of community burden in the assessment of development of such a policy.
So there is no data on any differences between vaccinated and unvaccinated health care workers. Yet these people are still arguing for VOM (vaccine or mask).
177. Dr. McGeer and Dr. Henry presented the position of the OHA and the Hospital based upon their understanding of the relevant literature. Neither of them asserted that they had particular expertise with respect to masks or had conducted studies testing masks.
So, no actual expertise of research. Bonnie Henry just read what was available. And this is the Provincial Health Officer of British Columbia.
219. Dr. Henry answered the ‘why not mask everyone’ question this way:
.
It is [influenza vaccination] by far, not perfect and it needs to be improved, but it reduces our risk from a hundred percent where we have no protection to somewhat lower. And there’s nothing that I’ve found that shows there’s an incremental benefit of adding a mask to that reduced risk…..there’s no data that shows me that if we do our best to reduce that incremental risk, the risk of influenza, that adding a mask to that will provide any benefit. But if we don’t have any protection then there might be some benefit when we know our risk is greater.
.
When we look at individual strains circulating and what’s happening, I think we need it to be consistent with the fact that there was nothing that gave us support that providing a mask to everybody all the time was going to give us any additional benefit over putting in place the other measures that we have for the policy. It’s a tough one. You know, it varies by season.[320]
.
It is a challenging issue and we’ve wrestled with it. I’m not a huge fan of the masking piece. I think it was felt to be a reasonable alternative where there was a need to do—to feel that we were doing the best we can to try and reduce risk.
.
I tried to be quite clear in my report that the evidence to support masking is not as great and it is certainly not as good a measure
Bonnie Henry admits no strong evidence to support maskings.
4. Henry Admits No Evidence Masks Work
Bonnie Henry admitted on January 30, 2020, that there’s no evidence to support the idea of putting masks on healthy people. See 0:22 in the video for the masks topic.
Note: as of yesterday, masks are now required on BC Transit, due largely to Bonnie Henry’s “new advice”. She is a complete fraud.
5. Bonnie Henry’s New Advice On Masks
Fast forward to July 24, and now Bonnie Henry now says that masks are beneficial to both healthy and sick people. Start at 1:00 in the video.
She says it’s about “courtesy and respect”.
Who knows what the next version will be?
Note: the man in the video is BC Health Minister Adrian Dix. Dix has no medical background whatsoever, (as he went to school for history and political science). Still, he is in this position of power.
6. Bonnie Henry Admits 30% False Negative Rate
Bonnie Henry admitted on April 13 that there is at least a 30% false negative rate in these tests. Apparently, you can be negative one moment, and then positive almost immediately afterwards.
B.C.’s provincial health officer says that mass testing continues to be an ineffective strategy to slow transmission of COVID-19 because it has a false negative rate as high as 30 per cent in people who are infected but don’t show symptoms.
At her daily briefing on Monday, Dr. Bonnie Henry said testing is not as sensitive as health officials expected it to be earlier in the crisis.
“The testing, unfortunately, doesn’t tell us the whole story. People can be negative one minute and positive within an hour.
“The false negative rate can be as high as 30 per cent early on in infection.”
Assuming Bonnie Henry is even telling the truth, these tests don’t actually work properly. Being positive but testing negative is not a sign that it’s accurate.
7. Bonnie Henry Admits High False Positive Rate
Henry said B.C.’s approach to testing is evolving based on epidemiology, testing capacity and methodology and a growing understanding of the virus.
She said routine testing of people -including those in schools, prior to surgery or other procedures, or as a condition of employment or for travel – is not recommended.
“It is important to understand that testing can result in false positive and false negatives, particularly in asymptomatic people and in people who are very early on in the illness or who may be incubating the disease,” Henry said in the letter.
She said serological tests for the virus causing COVID19 is recommended only to focus on informing the public health response and for clinical research investigations.
“If large numbers of false positive tests were to occur through routine testing of asymptomatic people, this could create a significant burden for the public health system and would provide little value in protecting your business and could impede our ability to protect the health of all British Columbians,” Henry said.
There would be large numbers of false positives? Wait a minute. Isn’t this test supposed to be highly accurate and reliable? How then would false positives overwhelm the medical system?
8. Barbara Yaffe Admits 50% False Positives
This was addressed in Part 43. Barbara Yaffe, Ontario’s Deputy Medical Health Officer, admits that there can be a 50% false positive error in PCR testing. She then bizarrely goes on to defend how important testing is. When asked about it, Premier Doug Ford talks in circles rather than give a straight answer.
For some context:
(a) BC admits there is a 30% false negative rate
(b) ON admits there is a 50% false positive rate
These tests are absolutely worthless.
9. BC CDC Has No Idea The Error Rate
5. What is the clinical sensitivity of the NAT test?
A statistic commonly quoted is that there is a 30% chance of a false negative result for a NAT test in a patient with COVID-19 infection (i.e., a 70% sensitivity). These and other similar estimates are based on a small number studies that compared the correlation between CT scan findings suggestive of COVID-19 infection to NAT on upper respiratory tract specimens. In these studies, 20-30% of people with a positive CT scan result had negative NAT results – and as discussed above a number of factors can contribute to false negative results. CT scan is not a gold standard for diagnosis of COVID-19 infection, and CT scan cannot differentiate amongst the many microbiological causes of pneumonia.
.
Ultimately, for COVID-19 testing, there is currently no gold standard, and the overall clinical sensitivity and specificity of NAT in patients with COVID-19 infection is unknown (i.e., how well NAT results correlate with clinical infection, “true positivity” or “true negativity” rate).
http://www.bccdc.ca/Health-Professionals-Site/Documents/COVID19_InterpretingTesting_Results_NAT_PCR.pdf
COVID19_InterpretingTesting_Results_NAT_PCR
10. Australia: PCR Tests Not Designed For This
Can reinfection occur?
There have been reports of apparent re-infection in a small number of cases. However, most of these describe patients having tested positive within 7-14 days after apparent recovery. Immunological studies indicate that patients recovering from COVID-19 mount a strong antibody response. It is likely that positive tests soon after recovery represent persisting excretion of viral RNA, and it should be noted that PCR tests cannot distinguish between “live” virus and noninfective RNA. Australian guidelines currently require patients who have had COVID-19 to test negative on two tests 24 hours apart before being released from isolation.
According to the Australian Health Department, positive tests are likely due to viral excretion. And the PCR tests cannot distinguish between that and live viruses. In spite of that, Australia has some of the most draconian measures on the planet.
If the Australian Government published this months ago, then why are these tests still being used? This is clearly not their intended purpose. Why doesn’t the BC Government know about this?
11. No Basis For Pandemic Declaration
Of course one has to ask WHY a vaccine is so critical, given how many people have already recovered. However, the obedient puppets in the media never seem to get to such details.
12. Henry Pushes Vaxx, Rejects Antibody Testing
Bonnie Henry dismisses the idea of widespread sampling for antibody testing. Instead, she once again pushes the idea that a vaccine is needed. See the comment at the end.
12. Henry Admits Antibody Testing Doesn’t Work

https://globalnews.ca/video/embed/7160788/”/
bonnie.henry.antibody.tests.false.positives.and.negatives.
And in this recent gem, BCPHO Bonnie Henry admits that there are lots of errors in antibody testing. This actually produces BOTH false positives and false negatives.
13. CDC And Accuracy Of Antibody Testing
Antibody testing is NOT recommended for:
.
The routine diagnosis of acute or recent COVID-19 infections. As antibodies can take 14 days or more to be reliably detected, and by 14 days after symptom onset most patients with COVID-19 infection are no longer considered infectious, serology provides limited information to guide immediate clinical or public health action. NAT remains the test of choice for diagnosis of acute COVID-19 infection. Furthermore as time passes and the SARS-CoV-2 virus continues to circulate, a positive antibody result may be due to a prior infection and not necessarily reflect the cause of an individual’s current symptoms.
Determining an individual’s immune status or past exposure. Antibody testing to document immunity to SARS-CoV-2 is NOT recommended as it has not yet been established whether the presence of antibodies provides protection from re-infection. It is also apparent that not everyone with past COVID-19 infection mounts a measurable antibody response that can be detected by laboratory testing, or for how long the antibodies persist. Therefore, antibody results cannot be used as proof of immunity for subsequent decision-making (e.g., decisions related to the use of personal protective equipment, adherence to physical distancing or other public health or workplace recommendations). Antibody testing is also not recommended to verify past exposure as a condition to employment or travel, in schools, prior to surgery or other medical procedures.
SO what’s the point of antibody testing if it can’t:
[1] Determine infection
[2] Determine immunity
[3] Be used to make medical decisions
http://www.bccdc.ca/health-professionals/clinical-resources/covid-19-care/covid-19-testing/antibody-testing-(serology)
https://archive.is/58jmq
http://www.bccdc.ca/Health-Professionals-Site/Documents/COVID19_SerologyTestingGuidelines.pdf
COVID19_SerologyTestingGuidelines
14. “Essential Businesses” Is Arbitrary List

In March, all “non-essential” businesses were ordered to close down by the BC Government. But how do they determine what is essential or not? How did they figure this was needed? Well, no real details were ever provided.
15. Bonnie Henry Openly Promotes Degeneracy
This is from Part 54. While she apparently doesn’t have a clue as to what is going on, the Provincial Health Officer still encourages all sorts of degenerate behaviour, as does the BC Center for Disease Control.
If these people weren’t actually in charge of the Province, this would be downright comical. As it is, it’s downright infuriating.
16. Who Are Bonnie Henry & Barbara Yaffe?
According to her LinkedIn profile, Barbara Yaffe graduated medical school in 1978, and was in various post-graduate programs until 1984. There is nothing listed until 1998, where she became a public health official in Toronto. She is registered with the CPSO, but there is no actual medical practice listed. So, why the almost 15 year gap?
Bonnie Henry appears to have graduated from medical school in 1990, and then spent another 11 years in school after that. She then went directly into being a Deputy Medical Officer with Toronto Public Health in 2001. So Henry and Yaffe were colleagues. There are 2 years of experience listed (2005 to 2007), but the overwhelming majority of her time seems to be in various political roles.
And was mentioned in Part 13, there is no record of Theresa Tam ever practicing medicine.
These are the people in charge of making public medical decisions.
Discover more from Canuck Law
Subscribe to get the latest posts sent to your email.
Hello! Quick question that’s totally off topic. Do you know how to make your site mobile friendly? My site looks weird when viewing from my apple iphone. I’m trying to find a theme or plugin that might be able to fix this problem. If you have any recommendations, please share. Thank you!
to whom it may concern. I am trying to get a hold of the actual arbitration that Bonnie Henry signed on in 2019, between BCNU and Health Employer Association of BC. that made it so masks are not mandated for aids and nurses to wear during flu season. I have contacted FOI and Health Ministry will not respond to them until Oct. I am now contacting privacy commissioner. I think its important that people see the evidence of this information. Let me know if anyone in your group has it. thank you
This woman will be tried at Nuremberg 2.0 trials. This is criminal.
After a lot of research I found that Bonnie Henry worked for the Bill Gates foundation for some years and is a ranking member of the “Eastern Star”, the female entity of the Free Masons, a known demonic cult. On one of her early TV interviews she war her cult badge on her lapel proudly displaying her dark side.
Can you show the research because I’ve been looking.
Eastern Star & Freemasons are certainly NOT a demonic cult. Where do you get your info from (Oh, wait, the internet, right?) My father and my husband were members. No devil worship took place.