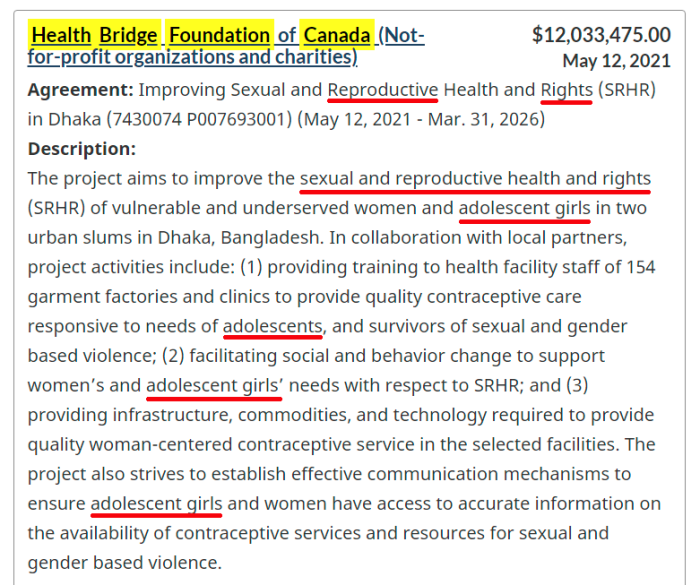
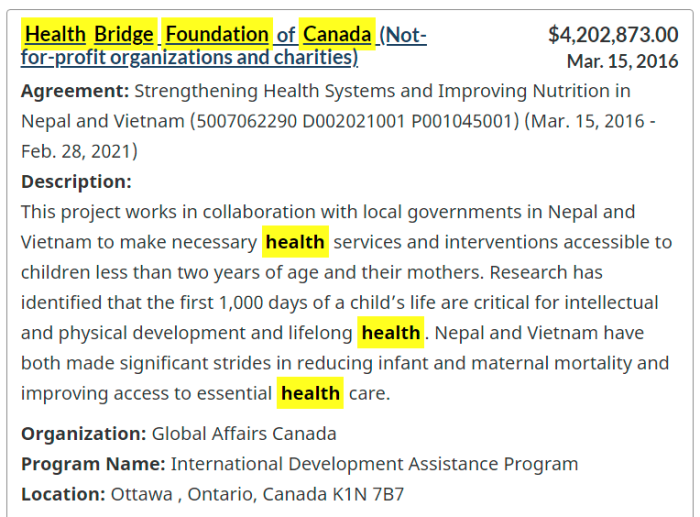
Health Bridge Foundation of Canada received $4.2 million from Canadian taxpayers in 2016. In 2021, there was the payment of another $12 million. While the first may not involve killing unborn children, the second certainly does. Now, if paying money to abort children abroad isn’t a worthwhile cause, then I don’t know what is. Even better, these programs will also target adolescents (girls) who are pregnant. Granted, there are other items spelled out in the grant, but killing children is one of them.
In the middle of a so-called global pandemic, it makes perfect sense to reduce the population as much as possible. Surely, we don’t need to be focusing on the preservation of human life, wherever possible. Please disregard the sarcasm.
Health Bridge is registered with the Canada Revenue Agency as a charity. This means that whenever someone in this country makes a donation, taxpayers are on the hook for about 45% to 50% of that total. That means that these grants are subsidized by the public, whether we agree or not.
2015 Tax Information From CRA
Receipted donations $50,053.00 (1.78%)
Non-receipted donations $36,402.00 (1.29%)
Gifts from other registered charities $1,133,209.00 (40.26%)
Government funding $662,181.00 (23.53%)
All other revenue $932,587.00 (33.14%)
Total revenue: $2,814,432.00
Charitable programs $2,385,454.00 (84.56%)
Management and administration $423,373.00 (15.01%)
Fundraising $12,198.00 (0.43%)
Political activities $0.00 (0.00%)
Gifts to other registered charities and qualified donees $0.00 (0.00%)
Other $0.00 (0.00%)
Total expenses: $2,821,025.00
2016 Tax Information From CRA
Receipted donations $26,260.00 (0.85%)
Non-receipted donations $25,065.00 (0.81%)
Gifts from other registered charities $738,550.00 (24.01%)
Government funding $863,745.00 (28.07%)
All other revenue $1,423,022.00 (46.25%)
Total revenue: $3,076,642.00
Charitable programs $2,600,136.00 (85.11%)
Management and administration $451,074.00 (14.77%)
Fundraising $3,689.00 (0.12%)
Political activities $0.00 (0.00%)
Gifts to other registered charities and qualified donees $0.00 (0.00%)
Other $2.00 (0.00%)
Total expenses: $3,054,901.00
2017 Tax Information From CRA
Receipted donations $51,582.00 (1.90%)
Non-receipted donations $62,941.00 (2.32%)
Gifts from other registered charities $688,456.00 (25.35%)
Government funding $1,105,668.00 (40.71%)
All other revenue $807,371.00 (29.73%)
Total revenue: $2,716,018.00
Charitable programs $2,257,162.00 (83.19%)
Management and administration $449,475.00 (16.57%)
Fundraising $6,589.00 (0.24%)
Political activities $0.00 (0.00%)
Gifts to other registered charities and qualified donees $0.00 (0.00%)
Other $0.00 (0.00%)
Total expenses: $2,713,226.00
2018 Tax Information From CRA
Receipted donations $38,250.00 (1.21%)
Non-receipted donations $49,002.00 (1.54%)
Gifts from other registered charities $790,541.00 (24.91%)
Government funding $990,245.00 (31.20%)
All other revenue $1,305,328.00 (41.13%)
Total revenue: $3,173,366.00
Charitable programs $2,703,713.00 (86.10%)
Management and administration $433,996.00 (13.82%)
Fundraising $2,402.00 (0.08%)
Political activities $0.00 (0.00%)
Gifts to other registered charities and qualified donees $0.00 (0.00%)
Other $0.00 (0.00%)
2019 Tax Information From CRA
Receipted donations $53,999.00 (1.49%)
Non-receipted donations $78,623.00 (2.17%)
Gifts from other registered charities $832,291.00 (23.00%)
Government funding $1,370,569.00 (37.88%)
All other revenue $1,283,116.00 (35.46%)
Total revenue: $3,618,598.00
Charitable programs $3,113,838.00 (87.78%)
Management and administration $433,244.00 (12.21%)
Fundraising $58.00 (0.00%)
Gifts to other registered charities and qualified donees $0.00 (0.00%)
Other $0.00 (0.00%)
Total expenses: $3,547,140.00
It would be nice to know what “all other revenue” really means. When it’s 30-40% or the total income, that’s quite the interesting bit of information. Now, who are those lovely people donating to the Health Bridge Foundation?
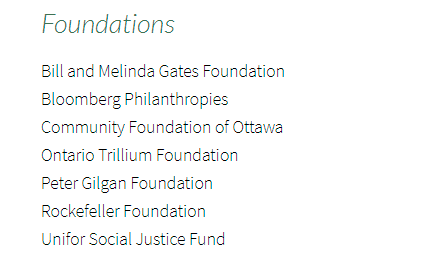
Don’t worry. Being supported by, and getting donations from places like the Bill & Melinda Gates Foundation, or the Rockefeller Foundation, are nothing to be concerned about. As for Unifor Social Justice, they are rocking the “Build Back Better” narrative, and its content seems eerily similar to the Great Reset.

HealthBridge Foundation of Canada (formerly PATH Canada) has been working since 1982 in Asia, Africa and the Americas. In the early years it undertook research and identified technologies and products that would improve contraception and health care in developing countries.
Since then, HealthBridge has evolved into an agile and efficient organization that aims to improve the health of vulnerable populations, including those at risk of malnutrition, infectious disease (particularly malaria and HIV/AIDS) and emerging epidemics, such as non-communicable diseases (NCDs).
HealthBridge is known for undertaking pioneering research, identifying and deftly addressing critical gaps in achieving health and health equity in the developing world, working effectively with local partners to bring about change in policy, and bridging the gap between service provider and service user.
All of this is cloaked as a health care initiative. However, it must be noted that one of the main services they offer involves promoting and facilitating abortion. This is apparently what passes for humanitarianism in our Government: neglecting the health care of Canadians, in order to finance genocide abroad.
Health Bridge also has a “livable cities” initiative. By itself, it wouldn’t sound so bad, except the climate change and UN Sustainable Development Agenda seems to creep in on it.
This NGO is headed by: (a) Eva Rathgeber, Adjunct Professor, University of Ottawa, who previously served on 2 UN groups; and (b) Carol Vlassoff, another University of Ottawa Professor, who spent 17 years working with the World Health Organization.
There we go. Another $12 million of taxpayer money (or additional debt) sent off to the 3rd World, to help reduce the population abroad. Doesn’t this feel so wonderful?
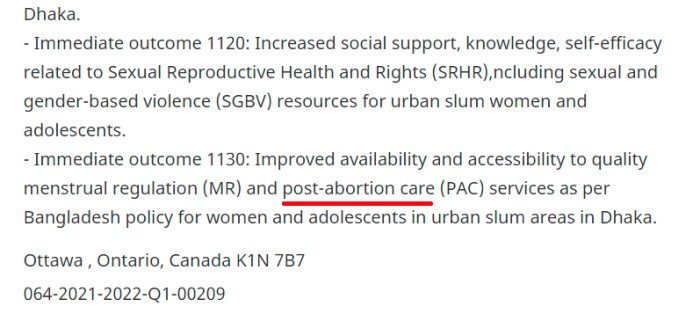
Just in case there is any ambiguity regarding the May 12, 2021 grant from the Canadian Government, “post abortion care” is explicitly listed as a function to be served. Yes, the term reproductive rights is a bit vague — probably on purpose — but abortion is put in there. It’s down near the bottom of the disclosure. Now, there will probably be other activities the money goes towards, but we are still financing the culling of people abroad.
Where are the so-called conservatives on this?
Thing is: probably no one reading this article had ever heard of Health Bridge previously. It’s not like the mainstream news outlets will cover such information. There’s no way to make this look good.
(1) https://healthbridge.ca/
(2) https://healthbridge.ca/page/our-supporters
(3) https://healthbridge.ca/page/our-story
(4) https://healthbridge.ca/programs/livable-cities
(5) https://healthbridge.ca/board/entry/dr.-eva-rathgeber
(6) https://healthbridge.ca/board/entry/dr-carol-vlassoff
(7) https://search.open.canada.ca/en/gc/?sort=score%20desc&page=1&search_text=HealthBridge%20Foundation%20of%20Canada
(8) https://search.open.canada.ca/en/gc/id/dfatd-maecd,064-2021-2022-Q1-00209,current
(9) https://apps.cra-arc.gc.ca/ebci/hacc/srch/pub/dsplyRprtngPrd?q.srchNm=health+bridge&q.stts=0007&selectedCharityBn=129950051RR0001&dsrdPg=1
(10) https://www.youtube.com/user/HealthBridgeCanada/videos