
Ever wonder why so many groups working the “levers of power” all seem to ideologically aligned with the same martial law measures? Think it’s strange that there is so little criticism or skepticism among prominent people and organizations? There is a simple explanation: FOLLOW THE MONEY!
(1) https://apps.cra-arc.gc.ca/ebci/hacc/cews/srch/pub/bscSrch
(2) https://apps.cra-arc.gc.ca/ebci/hacc/srch/pub/dsplyBscSrch?request_locale=en
(3) https://search.open.canada.ca/en/gc/
(4) https://lobbycanada.gc.ca/app/secure/ocl/lrs/do/advSrch
(A.1) Hotel, Restaurant Groups Getting Wage/Rental Subsidies
(A.2) Liberals, Conservatives, NDP All Getting Bailout Money
(A.3) Lawyers, Bar Associations Receiving CEWS Money
(A.4) Conflicting Out? Lawyers Getting More Than Just CEWS
(A.5) Churches Are Charities, Getting CEWS, Subsidies & Promoting Vaccines
(A.6) Trucking Alliance Grants Raising many Eyebrows
(A.7) Chambers Of Commerce Subsidized By Canadians, Want Open Borders
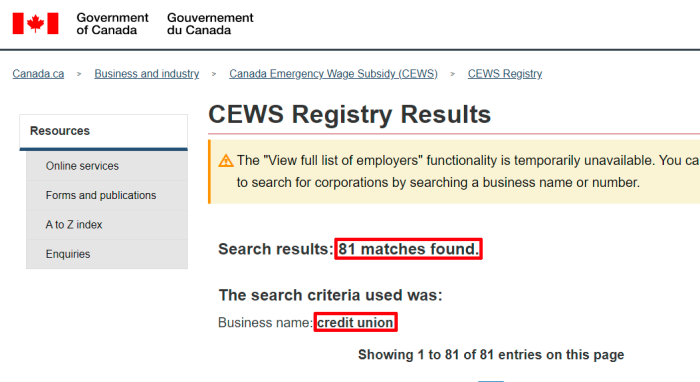
(A.8) Banks, Credit Unions, Media Outlets All Getting CEWS
(B.1) Unifor, Media, In Bed With Gov’t, $595M
(B.2) Government Subsidizes Media To Ensure Positive Coverage
(B.3) Postmedia Subsidies/Connections, Lack Of Real Journalism
(B.4) Latest “Pandemic Bucks” Grants In 2021, Lorrie Goldstein
(B.5) Nordstar; Torstar; Metroland Media; Subsidies & Monopoly
(B.6) Aberdeen Publishing Takes Handouts, Ignores Real Issues
(B.7) More Periodicals Taking Grants, Parroting Gov’t Narrative
(B.8) Tri-City News, LMP Pulls Bonnie Henry Article; Pandemic Bucks
(B.9) Black Press Group; Media Outlet Doxing Of Convoy Donors
(B.10) Subsidized Fact-Check Outlets Run By Political Operatives
(B.11) Digital Citizen Contribution Program: Funds To Combat “Misinformation”
(B.12) Counter Intelligence “Disinformation Prevention” Groups Are Charities
(B.13) CIVIX, More Grants To Combat “Disinformation” In 2021, Domestic, Foreign
(B.14) PHAC Supporting #ScienceUpFirst Counter Intel Effort
(B.15) Rockefeller Spends $13.5 To Combat Misinformation
(B.16) Media, Banks, CU, Getting CDA Emergency Wage Subsidies (CEWS)
(B.17) John Tory’s Sister Board Member At Bell; CEWS; Subsidies
(C.1) Media, Facebook, Google, Tech Collusion To Create “Trust” Networks
(C.2) CommonTrust, Commons Project, WEF, Rockefeller, Health Passes
(C.3) C2PA; Project Origin; Content Authenticity Initiative; CBC-BBC-Microsoft
(C.4) Public Media Alliance, Global Task Force, Brussels Declaration
(C.5) Institute For Strategic Dialogue: Govt/NGO Funded Counter-Intelligence
(C.6) Institute For Strategic Dialogue: Open Source Intelligence Gathering
(a) https://canucklaw.ca
(b) https://gab.com/canucklaw1
(c) https://twitter.com/Babylon_Beaver
(d) https://odysee.com/@CanuckLaw:8
(e) https://bitchute.com/channel/canuck_law
(f) https://rumble.com/user/CanuckLaw
(g) https://www.youtube.com/c/CanuckLawVids