
Remember the hype in 2022 about a a proposed Global Pandemic Treaty? This was supposed to be an agreement that would give the World Health Organization binding legal authority over elected Governments. That seems to have stalled, at least to the casual observer.
Of course, the W.H.O. already has binding legal authority over Member States, which includes Canada. Anyone who’s ever read their Constitution would know that. That said, it doesn’t stop politicians from slipping in their rules in domestic legislation.
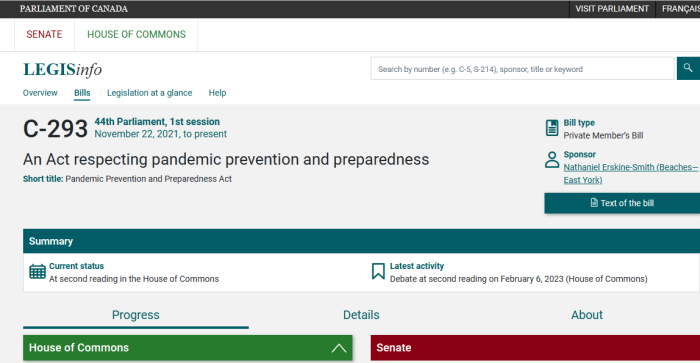
Private Member’s Bill C-293 was sponsored by Liberal M.P. Nathaniel Erskine-Smith (Beaches—East York). The content of which is interesting, to say the least.
Most Private Bills don’t become law. However, their content may become embedded into other legislation, and rammed through without proper debate and consideration.
Erskine-Smith isn’t a big player in Canadian politics. So, it’s strange that he would introduce something like this. Have to wonder if he wrote any of it.
Preamble
Whereas the costs of prevention and preparedness measures are insignificant in comparison to the human and economic costs of a pandemic;Whereas Parliament is committed to making efforts to prevent the risk of and prepare for future pandemics and to promote transparency and accountability in relation to those efforts;
Whereas it is critical to build on the lessons learned from previous outbreaks of serious diseases, including severe acute respiratory syndrome (SARS), Ebola virus disease (EVD), Zika virus disease, tuberculosis, H1N1 flu and coronavirus disease 2019 (COVID-19);
Whereas a One Health approach — a multisectoral and multidisciplinary collaborative approach that focuses on the human, animal, plant and ecosystem health and welfare interface — is central to preventing the risk of future pandemics;
And whereas this approach requires sustained collaboration among various ministers, all levels of government and Indigenous communities;
Now, therefore, Her Majesty, by and with the advice and consent of the Senate and House of Commons of Canada, enacts as follows:
There is something of a bait-and-switch here. While the Bill is presented as cooperation between various Governments in Canada, it’s clear that it also involves supra-national control.
Plan — contents
(2) The pandemic prevention and preparedness plan must
(a) set out a summary of mitigation strategies that the Minister of Health intends to implement in order to prevent the risk of and prepare for disease outbreaks that could lead to pandemics, as well as a projected timeline for their implementation;
Should we just state the obvious? They aren’t preparing for future outbreaks. Instead, this is laying the groundwork to erase more of people’s rights under the pretext of an outbreak.
(iv) the surge capacity of human resources required for the testing and contact tracing of persons exposed to infectious diseases, and
Contact tracing is just a means to implement mass surveillance.
(i) the manufacturing capacity in Canada with respect to any product relevant to pandemic preparedness, including vaccines, testing equipment and personal protective equipment, and the measures that the Minister of Industry intends to take to address any supply chain gaps identified, and
Expect more taxpayer money to be pumped into “building up reserves”, regardless of whether such items would ever be used. Think of the millions of vaccines that are going to waste.
(ii) the communications capacity and infrastructure for electronic platforms and tools, including electronic applications that enable contact tracing of persons exposed to infectious diseases that could lead to pandemics;
Building the infrastructure for electronic monitoring of “infected” people?! Canada already has a system in place to track people on parole and probation. Why would such an expansion be necessary, unless they were anticipating a massive influx?
(ii) regulate commercial activities that can contribute to pandemic risk, including industrial animal agriculture,
(iii) promote commercial activities that can help reduce pandemic risk, including the production of alternative proteins, and
Going back to the 2017 Federal Budget, millions were pumped into the “alternative protein” industry. Considering that this Bill also talks about reducing natural agriculture, a cynic may wonder if this is done to force citizens to take these alternative “foods”.
(iv) phase out commercial activities that disproportionately contribute to pandemic risk, including activities that involve high-risk species;
The suggestion has been made many times before, that this can be used as an excuse to attack the food supply. As such, the public would be forced to starve, or seek other alternative foods.
(m) include the following information, to be provided by the Minister of the Environment:
(i) after consultation with relevant provincial ministers, a summary of changes in land use in Canada, including in relation to disturbed habitats, that could contribute to pandemic risk, such as deforestation, encroachment on wildlife habitats and urbanization and that were made, in the case of the first plan, since the last report on changes in land use published under the Federal Sustainable Development Act or, in the case of the updated plans, during the reporting period for the updated plan,
This is essentially merging the U.N. Sustainable Development Agenda with the W.H.O.’s goals. Sorts of sounds like the GREAT RESET, which was just a conspiracy theory.
(ii) a summary of the measures the Minister of the Environment intends to take to reduce the risk that the commercial wildlife trade in Canada and abroad will lead to a pandemic, including measures to regulate or phase out live animal markets, and
Phase out live animal markets? Is this a way to help manufacture a food shortage? Could this be done by claiming that entire farms are “at risk”, and then culling them to protect the public?
(n) include a summary, to be provided by the Minister of Foreign Affairs, of the measures that that minister intends to take to support global health equity, including measures to increase public health capacity around the world and to ensure equitable access to vaccines, testing equipment and treatment;
(o) set out, in consultation with relevant ministers, a summary of key cooperative measures or agreements on disease outbreak prevention and preparedness between the Government of Canada, other foreign governments and key international organizations, including the World Health Organization, the United Nations Environment Programme, the World Organization for Animal Health and the Food and Agriculture Organization of the United Nations; and
Here’s where it hits home. This will not simply be a Canadian system. Instead, it will be done in collaboration with:
- Foreign Governments
- World Health Organization
- United Nations Environment Programme
- U.N. Animal Health and the Food and Agriculture Organization
Read the entire Bill to make sure that nothing is being taken out of context. But this looks like a way to slip even more draconian measures onto the public.
And again, there has been — to my knowledge — any debate or reporting on this Bill. Why exactly is that? Isn’t this in the public interest?
1908: International Public Health Office to be created
1926: International Sanitary Convention was ratified in Paris.
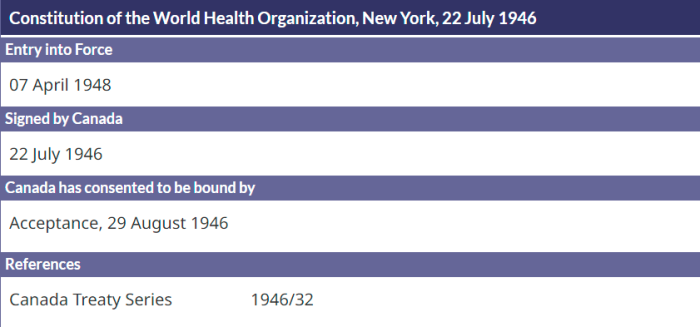
1946: WHO’s Constitution was signed, and it’s something we’ll get into in more detail.
1951: International Sanitary Regulations adopted by Member States.
1969: International Health Regulations (1st Edition) replaced ISR. These are legally binding on all Member States.
2005: International Health Regulations 3rd Edition of IHR were ratified.
Without regurgitating the whole thing, the W.H.O. Constitution has been covered before, including the fact that it’s legally binding on Member States.
As has been outlined here before, the 2005 Quarantine Act, Bill C-12, was really just domestic implementation of the 3rd Edition of the International Health Regulations.
We’ve also gone heavily into the creation of PHAC, which is essentially just a branch of the World Health Organization. It was created at WHO’s instigation. It takes over (to a large degree) what Health Canada had been doing. The timeline is laid out, and worth a read.
Why does an unknown like Nathaniel Erskine-Smith introduce such a Bill? According to his Wikipedia page, he’s actually brought forward several pieces. This included (in the last Parliament) Bill C-235 to delete the drug possession offence from the Criminal Code. He also brought Bill C-236, to expand diversion alternatives for criminal cases involving drugs.
Whether or not this “Pandemic Treaty” ever goes ahead, this legislation seems designed to carry out the goals it was intended for. Perhaps this should be put to a public debate.
Again, why is this being done quietly in a Private Member’s Bill?
(1) https://eppc.org/publication/the-whos-pandemic-treaty/
(2) WHO Constitution, Full Document
(3) https://www.who.int/about/governance/constitution
(4) https://www.parl.ca/legisinfo/en/bills?chamber=1&page=3
(5) https://www.parl.ca/legisinfo/en/bill/44-1/c-293
(6) https://www.ourcommons.ca/Members/en/nathaniel-erskine-smith(88687)
(7) https://en.wikipedia.org/wiki/Nathaniel_Erskine-Smith
(8) https://www.parl.ca/legisinfo/en/bill/43-1/c-235
(9) https://www.parl.ca/legisinfo/en/bill/43-1/c-236