
It was reported back in July 2022 that 2 high profile anti-lockdown lawsuits in Canada hadn’t seemed to go anywhere in well over a year.
(a) bodily autonomy of police officers, organized by Police on Guard
(b) children’s rights and masks in Ontario schools, organized by Children’s Health Defense (Canada)
Both were filed in April 2021. After some initial hype in the alternative media, there were no updates to report. As we enter 2023, and approach the 2 year anniversary, it appears that there’s still nothing to write back about.
Even though (most) of the Respondents now are represented by lawyers, it looks like nothing has happened to the cases themselves. There have been no Motions, evidence sworn or hearings so far.
Interestingly, while no Motion to Strike has been brought, there was a Rule 2.1.01(6) request filed in May of 2021 for the CHDC case. That seems odd, as it isn’t really the best mechanism for getting such a case thrown out.
Both organizations are still asking for donations, and it’s implied that at least portions of those funds would be used towards these Court cases.
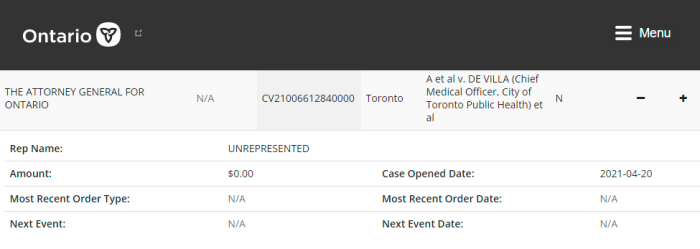
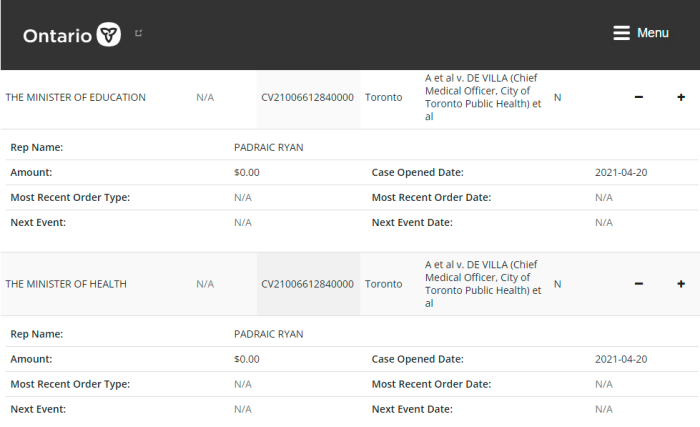
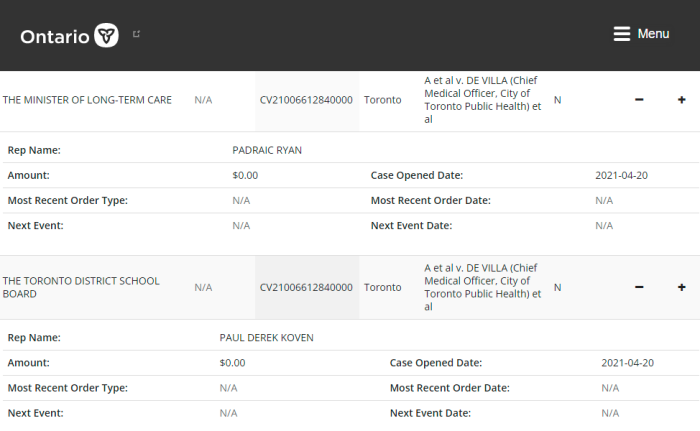
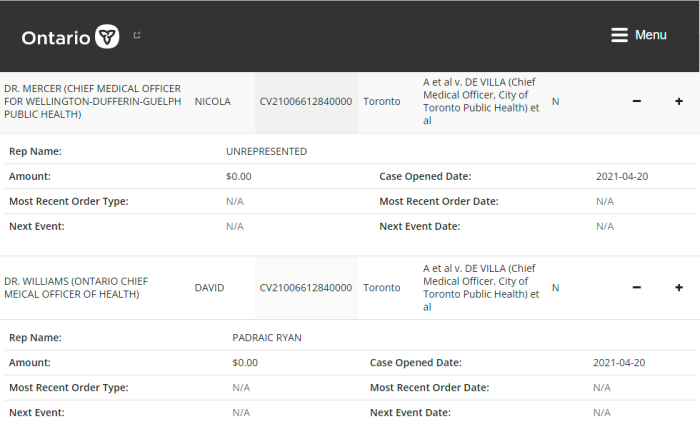
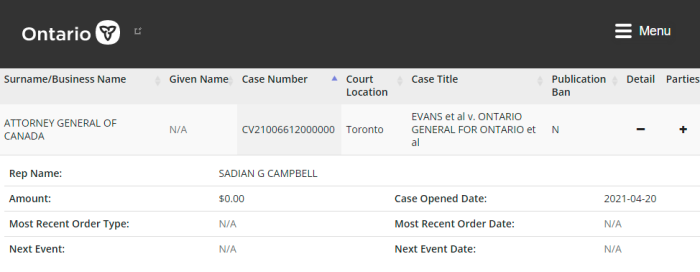
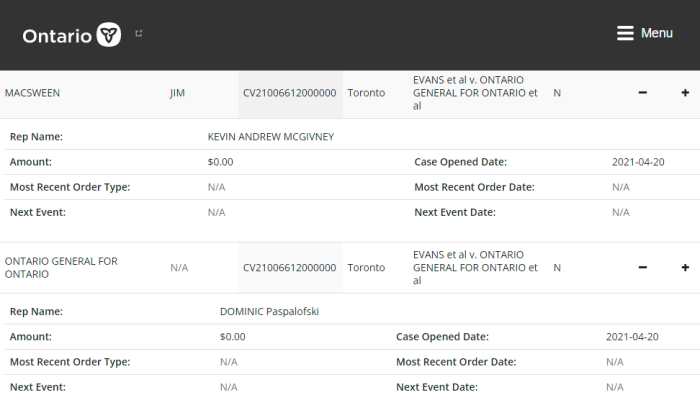
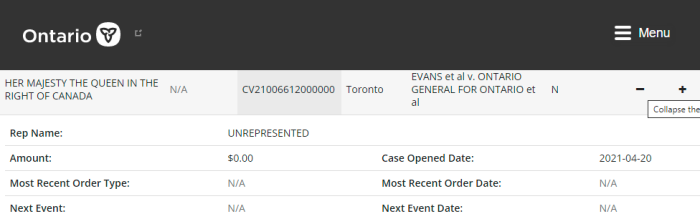
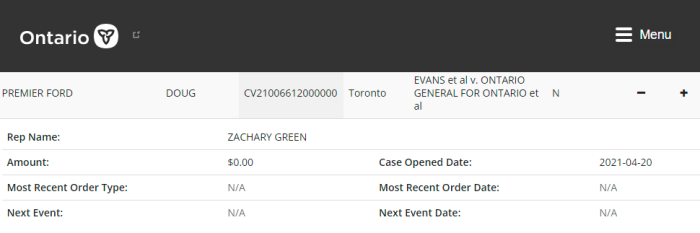
As is shown by the Court records, there are no previous Orders that have been handed down in either case. Nor are any hearings scheduled as of now.
Of course, members of the public can SEARCH FOR FREE as to the updates on such cases. Instead of taking the word of people who have incentives to drive fundraising — or some reporter on the internet — go check the cases for yourselves.
Ontario Superior Court, Civil Branch
330 University – Toronto
330 University Ave.
Toronto ON M5G 1R7
Court file#: (plug in the file number)
Civil – Superior Court of Justice
tel. 416-327-5440 (front desk)
CSD.SCJRecords(at)ontario.ca (records department)
It’s worth noting that the POG Application and the CHDC Applications are almost identical. It’s as if one was cut-and-pasted into the other, with the facts and names changed.
Why keep reporting on this? Because they are public cases, and public donations are — still — being solicited. People have a right to know what’s happening, and what’s not happening.
(1) https://www.ontario.ca/page/search-court-cases-online
POLICE ON GUARD/OFFICERS:
(1) Notice Of Application — April 20, 2021
POLICE ON GUARD CORPORATE DOCUMENTS:
(1) Police On Guard Incorporation
(2) Police On Guard Registered Office & Directors
(3) Police On Guard Directors
(4) Police On Guard Bylaws
(5) Police On Guard Directors Later
ONTARIO STUDENTS/CHDC:
(1) Notice Of Application — April 20, 2021, Masks On Students
(2) Schools – Rule 2.1.01 Decision
(3) Schools — Notice Of Appearance Robert Kyle
(4) Schools — Notice Of Appearance Halton Durham
CHD CANADA CORPORATE DOCUMENTS:
(1) Childrens Health Defense Canada Registered Office
(2) Childrens Health Defense Canada Incorporation
(3) Childrens Health Defense Registered office & Directors
(4) Childrens Health Defense Canada Annual Return