
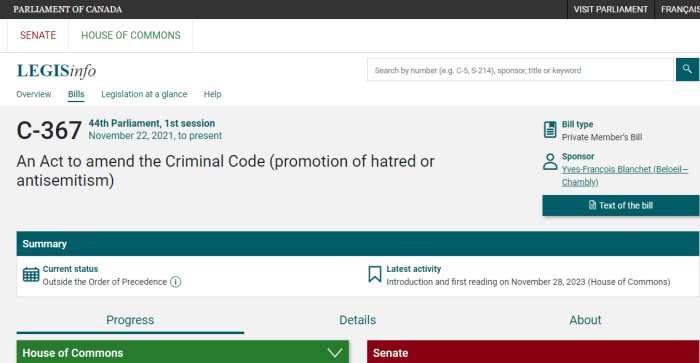
A Private Member’s Bill is getting renewed expression for the potential impact it may have. Bill C-367 would remove “belief based on a religious text” as a defence to certain criminal charges.
The text of the Bill would remove both sections 319(3)(b) and 319(3.1)(b) from the Criminal Code of Canada. Those provisions provide legal defences to people charged with the willful promotion of antisemitism, if it’s done in the context of religious expression. Truth is still allowed, for now.
Of course, the vagueness of these hate speech laws is already an issue. Nothing is properly defined, which makes it very subjective. But remove a potential justification? That’s worth a closer look.
Defences
.
(3) No person shall be convicted of an offence under subsection (2)
(a) if he establishes that the statements communicated were true;
(b) if, in good faith, the person expressed or attempted to establish by an argument an opinion on a religious subject or an opinion based on a belief in a religious text;
(c) if the statements were relevant to any subject of public interest, the discussion of which was for the public benefit, and if on reasonable grounds he believed them to be true; or
(d) if, in good faith, he intended to point out, for the purpose of removal, matters producing or tending to produce feelings of hatred toward an identifiable group in Canada.
Defences — subsection (2.1)
.
(3.1) No person shall be convicted of an offence under subsection (2.1)
(a) if they establish that the statements communicated were true;
(b) if, in good faith, they expressed or attempted to establish by an argument an opinion on a religious subject or an opinion based on a belief in a religious text;
(c) if the statements were relevant to any subject of public interest, the discussion of which was for the public benefit, and if on reasonable grounds they believed them to be true; or
(d) if, in good faith, they intended to point out, for the purpose of removal, matters producing or tending to produce feelings of antisemitism toward Jews.
This came from Yves-François Blanchet, the leader of the Bloc Québécois.
Blanchet is also on a large number of international associations in Parliament. This is rather strange, considering his stated goal of breaking up Canada. These people larp as if Quebec were an independent country, and it’s taken seriously.
- (CAAF) Canada-Africa Parliamentary Association
- (CACN) Canada-China Legislative Association
- (CADE) Canada-Germany Interparliamentary Group
- (CAEU) Canada-Europe Parliamentary Association
- (CAFR) Canada-France Inter-Parliamentary Association
- (CAIE) Canada-Ireland Interparliamentary Group
- (CAIL) Canada-Israel Interparliamentary Group
- (CAIT) Canada-Italy Interparliamentary Group
- (CAJP) Canada-Japan Inter-Parliamentary Group
- (CANA) Canadian NATO Parliamentary Association
- (CAPF) Canadian Branch of the Assemblée parlementaire de la Francophonie
- (CCOM) Canadian Branch of the Commonwealth Parliamentary Association
- (CEUS) Canada-United States Inter-Parliamentary Group
- (CPAM) Canadian Section of ParlAmericas
- (RUUK) Canada-United Kingdom Inter-Parliamentary Association
- (SECO) Canadian Delegation to the Organization for Security and Co-operation in Europe Parliamentary Assembly
- (UIPU) Canadian Group of the Inter-Parliamentary Union
Considering Blanchet’s position, it’s not really that surprising who paid him a visit recently.
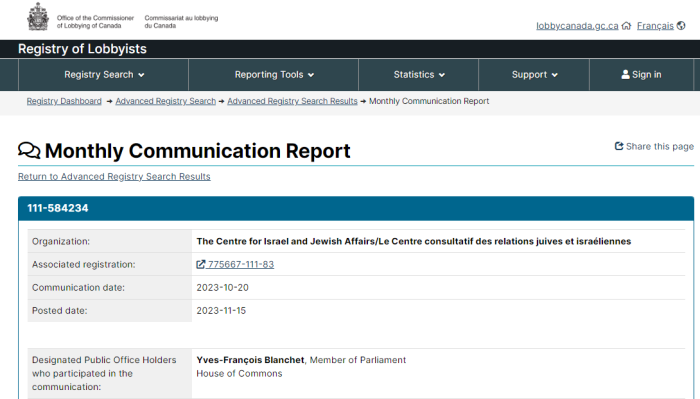
October 20th, 2023, Blanchet gets lobbied by CIJA, the Centre for Israel and Jewish Affairs. November 28th, he introduces Bill C-367 in Parliament. That’s less than 6 weeks later.
Quebec is largely a Catholic province — although immigration is replacing that — so it’s really odd that Blanchet would introduce this Bill. His own constituents could be impacted by this, depending on how it’s interpreted and enforced.
Interestingly, even those who cover the Bill omit the CIJA angle. The Christian Heritage Party, CHP, has commented on Bill C-367 being introduced in late 2023, but no mention of the lobbying behind the scenes. Lifesite ignores it as well. So does at least one pastor.
CIJA is very prolific in Canadian politics.
Their profile lists the following:
- Digital Citizen Contribution Program (DCCP): The objective of the project is to combat online disinformation and hate, specifically, antisemitism and antisemitic conspiracy theories related to COVID-19 where it is spreading: online via social media. Antisemitism cannot be allowed to permeate civil discourse and become mainstream
- A civil remedy based in human rights law, included in the Canadian Human Rights Act, with respect to combating hate speech, including antisemitism. Training for provincial attorneys general, prosecutors, and police to enforce Criminal Code hate speech provisions. Training and parameters should cite the International Holocaust Remembrance Alliance working definition of antisemitism.
- Civil remedy included in the Canadian Human Rights Act with respect to combating antisemitism.
- Equip police departments to counter hate crimes and support targeted communities by providing additional resources to bolster existing police hate crime and community liaison units. Where such units do not exist, funding should be provided to establish them.
- Update the Criminal Code of Canada with respect to combating antisemitism and online hate. Create a national strategy to tackle online hate and radicalization using the 2019 Justice Committee report, “Taking Action to End Online Hate”, as a foundation. A strategy should draw upon the Christchurch Call, and use the International Holocaust Remembrance Alliance definition of antisemitism.
- Hate speech and internet-based hate: For Canada to adopt policies – either/and through legislation or policies adjustments that will provide measurable standards for internet-based dissemination of hate speech, including explicit provisions within the Crimical Code and/or the Human Rights Act.
There are, of course, many other areas CIJA advocates for, such as ending the blood ban for gays. However, a large portion of the focus seems to be around speech and expression.
Don’t expect so-called “Conservatives” to come to the aid of principled free speech. They quite enthusiastically introduced Bill C-250, to jail people for questioning the official version of WWII.
Bill C-250 became moot when the equivalent provisions passed, slipped into Bill C-19, a budget Bill. Nonetheless, there was no pushback or resistance from the political right in Canada. And this highlights the hypocrisy they engage in.
Conservatives were outraged — or at least they pretended to be — over M-103, which was Iqra Khalid’s Motion to “study Islamophobia”. They railed that it was a waste of money, and an attack on free speech. And it was. That being said, they’re supportive of other attempts to imprison Canadians for having incorrect views on history.
News of Bill C-250 was announced on the CPC website, but has since been taken down. However, it has been archived and saved.
This new Bill aims to remove a protection that had previously been embedded in the last one. Incrementalism seems to be the way in politics.
(1) https://www.parl.ca/legisinfo/en/bill/44-1/c-367
(2) https://www.ourcommons.ca/Members/en/yves-francois-blanchet(104669)
(3) https://www.parl.ca/diplomacy/en/groups/cail
(4) https://www.parl.ca/documentviewer/en/IIA/constitution/8385503
(5) https://www.parl.ca/DocumentViewer/en/44-1/bill/C-367/first-reading
(6) https://twitter.com/CHPCanada/status/1760773690902401300/
(7) https://www.lifesitenews.com/opinion/proposed-canadian-law-could-see-christians-jailed-for-quoting-the-bible/
(8) https://twitter.com/aylmerpastor/status/1760787350496395632
(9) https://www.conservative.ca/mp-waugh-introduces-legislation-to-prohibit-holocaust-denial/
(10) https://archive.ph/fCnNn
(11) MP Waugh introduces legislation to prohibit Holocaust denial – Conservative Party of Canada
(12) Wayback Machine On Bill C-250
Private Member Bills In Current Session:
(A) Bill C-206: Decriminalizing Self Maiming To Avoid Military Service
(B) Bill C-207: Creating The “Right” To Affordable Housing
(C) Bill C-219: Creating Environmental Bill Of Rights
(D) Bill C-226: Creating A Strategy For Environmental Racism/Justice
(E) Bill C-229: Banning Symbols Of Hate, Without Defining Them
(F) Bill C-235: Building Of A Green Economy In The Prairies
(G) Bill C-245: Entrenching Climate Change Into Canada Infrastructure Bank
(H) Bill C-250: Imposing Prison Time For Holocaust Denial
(I) Bill C-261: Red Flag Laws For “Hate Speech”
(J) Bill C-293: Domestic Implementation Of Int’l Pandemic Treaty
(K) Bill C-312: Development Of National Renewable Energy Strategy
(L) Bill C-315: Amending CPPIB Act Over “Human, Labour, Environmental Rights”
(M) Bill S-215: Protecting Financial Stability Of Post-Secondary Institutions
(N) Bill S-243: Climate Related Finance Act, Banking Acts
(O) Bill S-248: Removing Final Consent For Euthanasia
(P) Bill S-257: Protecting Political Belief Or Activity As Human Rights