

Today’s topic concerns Danielle Smith, running to become Premier of Alberta. She used to be the head of the Wildrose Party in that Province.
Why go after someone who claims to be fighting for freedom, at least in Alberta? Because there are critical topics that are going unsaid.
In fairness, ideas like setting up a Provincial police force (like the O.P.P.), and doing local tax collection are interesting.
While Smith’s campaign seems to be starting well, there are plenty of red flags. Specifically, there are concerns that she doesn’t appear to be addressing. Her rise also seems controlled and inorganic, much like that of Poilievre.
Of course, if these things were properly addressed, than an apology is warranted. But they don’t seem to have been.
For starters, Smith (and all Western “conservatives”) claim to want to rebuild the oil & gas sector. However, they ignore the fact that Agendas 21 and 2030 make it clear these industries are to be killed off. These were signed by Mulroney and Harper respectively.
Smith is running for the leadership of the United Conservative Party, which Jason Kenney is leaving. In launching her campaign, she goes on about how Alberta needs to be protected from Trudeau. Of course, this applies to Ottawa more generally.
What makes this ring hollow is that the UCP received the wage subsidy, CEWS, for at least a portion of the last 2 years. It’s pretty hard to be against the Trudeau regime when his programs are paying your organization’s bills.
While Jason Kenney claimed to be resisting tyranny in Ottawa, his party was sucking at the teet of Federal bailout programs.
It’s a great talking point to be challenging Trudeau on “vaccinations” for certain things, but it completely glosses over the fact that Kenney brought in a Provincial system in late 2021, despite repeatedly promising not to. Smith is also running to head the party that was too spineless to stop Kenney, Hinshaw and Shandro.
Of course, the UCP is hardly alone in being bought off. The Alberta Liberals also got the subsidies, as did the Federal Liberals, Conservatives, and NDP. Watch the original video, or the remake for a look at the rot in our system.
There’s also no mention about the rampant pharma lobbying trying to influence policies in Alberta. Yes, it happens everywhere, but it’s not exactly a secret.
If Smith was serious about freedom and sovereignty for Alberta, she could always have thrown Kenney under the bus for his World Economic Forum connection. Either she doesn’t know about it, or just chose not to do so.
For obvious reasons, anyone tied to that organization can never be trusted to put their constituents first.
| YEAR END | TOTAL REVENUE | NON-GOV’T | PERCENTAGE |
|---|---|---|---|
| March 2017 | $14,325,881,000 | $922,364,000 | 6.54% |
| March 2018 | $13,780,984,000 | 0 | 0% |
| March 2019 | $15,134,433,000 | $948,317,000 | 6.27% |
| March 2020 | $15,335,736,000 | $971,471,000 | 6.33% |
| March 2021 | $16,489,501,000 | $767,768,000 | 4.66% |
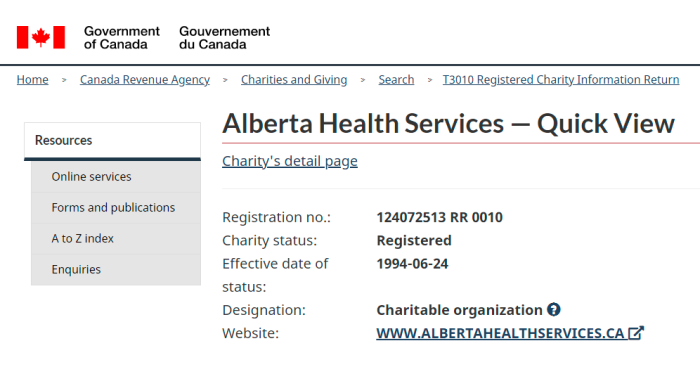
Alberta Health Services is a registered charity, according to the Canada Revenue Agency. Although 2017/2018 seems to be an anomaly, A.H.S. takes close to $1 billion/year from non-Governmental sources. It would be nice to know who these are.
Not only are private organizations allowed to donate, and potentially influence policy, taxpayers are forced to subsidize those donations. Tax credits amount to approximately 40% – 50% of the contributions.
Worth mentioning: this site has asked the C.R.A. several times for donor information. However, those requests were refused, citing privacy protections.
Pretty hard to do a proper job of criticizing A.H.S. while leaving this out.
In order for Alberta to have control over its affairs, it’s important to know what international agreements various Federal Governments have signed over the years. Smith doesn’t appear to have addressed any of this. As such, she’s in no position to offer such things, even if she were Premier.
Over a century ago, an International Public Health Office was created, which we became a part of. This was done without any democratic mandate of course.
1926: International Sanitary Convention was ratified in Paris.
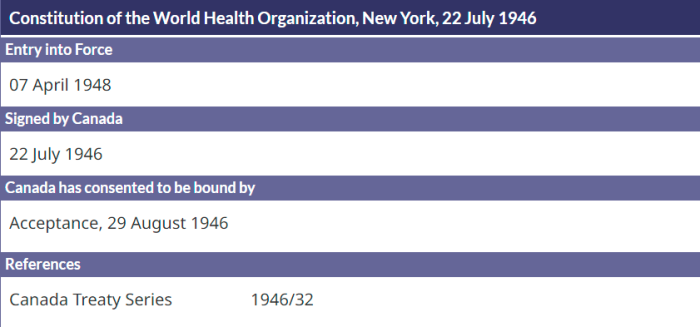
1946: WHO’s Constitution was signed, and it’s something we’ll get into in more detail.
1951: International Sanitary Regulations adopted by Member States.
1969: International Health Regulations (1st Edition) replaced ISR. These are legally binding on all Member States.
2005: International Health Regulations 3rd Edition of IHR were ratified.
In order to be part of the World Health Organization, it means adopting their Constitution, and ceding a large amount of sovereignty to an international body. No prominent politicians in Canada of any stripe have addressed this point. Are they all controlled?
Article 4
Members of the United Nations may become Members of the Organization by signing or otherwise accepting this Constitution in accordance with the provisions of Chapter XIX and in accordance with their constitutional processes.
Article 19
The Health Assembly shall have authority to adopt conventions or agreements with respect to any matter within the competence of the Organization. A two-thirds vote of the Health Assembly shall be required for the adoption of such conventions or agreements, which shall come into force for each Member when accepted by it in accordance with its constitutional processes.
Article 20
Each Member undertakes that it will, within eighteen months after the adoption by the Health Assembly of a convention or agreement, take action relative to the acceptance of such convention or agreement. Each Member shall notify the Director-General of the action taken, and if it does not accept such convention or agreement within the time limit, it will furnish a statement of the reasons for non-acceptance. In case of acceptance, each Member agrees to make an annual report to the Director-General in accordance with Chapter XIV
Article 21
The Health Assembly shall have authority to adopt regulations concerning:
(a) sanitary and quarantine requirements and other procedures designed to prevent the international spread of disease;
(b) nomenclatures with respect to diseases, causes of death and public health practices;
(c) standards with respect to diagnostic procedures for international use;
(d) standards with respect to the safety, purity and potency of biological, pharmaceutical and similar products moving in international commerce;
(e) advertising and labelling of biological, pharmaceutical and similar products moving in international commerce.
Article 22
Regulations adopted pursuant to Article 21 shall come into force for all Members after due notice has been given of their adoption by the Health Assembly except for such Members as may notify the Director-General of rejection or reservations within the period stated in the notice.
Being part of the World Health Organization means submitting to their rules and control. It’s laid out in their own constitution. To be clear, sovereignty will never be possible as long as Canada is part of this entity.
As has been outlined here before, the 2005 Quarantine Act, Bill C-12, was really just domestic implementation of the 3rd Edition of the International Health Regulations.
We’ve also gone heavily into the creation of PHAC, which is essentially just a branch of the World Health Organization. It was created at WHO’s instigation. The timeline is laid out, and worth a read.
Isolation, Quarantine and Special Measures
.
Isolation and quarantine
.
29(1) A medical officer of health who knows of or has reason to suspect the existence of a communicable disease or a public health emergency within the boundaries of the health region in which the medical officer of health has jurisdiction may initiate an investigation to determine whether any action is necessary to protect the public health.
(2) Where the investigation confirms the presence of a communicable disease, the medical officer of health
(a) shall carry out the measures that the medical officer of health is required by this Act and the regulations to carry out, and
(b) may do any or all of the following:
(i) take whatever steps the medical officer of health considers necessary
(A) to suppress the disease in those who may already have been infected with it,
(B) to protect those who have not already been exposed to the disease,
(C) to break the chain of transmission and prevent spread of the disease, and
(D) to remove the source of infection;
(ii) by order
(A) prohibit a person from attending a school,
(B) prohibit a person from engaging in the person’s occupation, or
(C) prohibit a person from having contact with other persons or any class of persons for any period and subject to any conditions that the medical officer of health considers appropriate, where the medical officer of health determines that the person’s engaging in that activity could transmit an infectious agent;
.
(iii) issue written orders for the decontamination or destruction of any bedding, clothing or other articles that
have been contaminated or that the medical officer of health reasonably suspects have been contaminated.
(2.1) Where the investigation confirms the existence of a public health emergency, the medical officer of health
(a) has all the same powers and duties in respect of the public health emergency as he or she has under subsection (2) in the case of a communicable disease, and
(b) may take whatever other steps are, in the medical officer of health’s opinion, necessary in order to lessen the impact of the public health emergency.
A serious candidate would vow to scrap the Alberta Public Health Act, or at least gut it. This legislation (and all Provinces have a similar version) are derived from the 2005 Quarantine Act, which itself came from WHO’s International Health Regulations.
It makes no sense to propose an Alberta Sovereignty Act, while leaving intact the legislation which signs away the Province’s control in the first place.
On November 30, 2020, Smith interviewed Kenney for the show she had at the time. The clip starts at about 28:30 in the full recording. Smith made it pretty clear she’s quite able to do research.
She also brought up the issue of 90% false positives for PCR testing (notwithstanding the fact that no virus exists). Even 18 months ago, she clearly knew that this “pandemic” was a scam. But that person seems to have vanished.
Much like Ron DeSantis of Florida, Smith will scream about bodily autonomy, all while ignoring or downplaying the obvious psy-op over the last few years. This was planned and deliberate, not just some collective incompetence.
A cynic would view all of this as a candidate dropped in to placate the masses. A more charitable interpretation would be a total lack of understanding of what’s going on.
Now, could Smith be a decent Premier? Maybe. However, she leaves out so much that it’s hard to see her as anything but another fake freedom fighter.
(1) https://twitter.com/ABDanielleSmith
(2) https://twitter.com/ABDanielleSmith/status/1544454483388014593/
(3) https://apps.cra-arc.gc.ca/ebci/habs/cews/srch/pub/bscSrch
(4) https://www.bitchute.com/video/WooZ4LCmdDs5/
(5) https://www.weforum.org/people/jason-t-kenney
(6) https://apps.cra-arc.gc.ca/ebci/hacc/srch/pub/dsplyBscSrch?request_locale=en
(7) https://apps.cra-arc.gc.ca/ebci/hacc/srch/pub/dsplyRprtngPrd?q.srchNmFltr=alberta+health+services&q.stts=0007&selectedCharityBn=124072513RR0010&dsrdPg=1
(8) https://www.treaty-accord.gc.ca/index.aspx
(9) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=103984&t=637793587893732877
(10) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=103986&t=637862410289812632
(11) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=103990&t=637793587893576566
(12) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=103994&t=637862410289656362
(13) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=103997&t=637793622744842730
(14) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=105025&t=637793622744842730
(15) https://canucklaw.ca/wp-content/uploads/WHO-Constitution-Full-Document.pdf
(16) https://canucklaw.ca/cv-62g-public-health-agency-of-canada-created-as-branch-of-who-bill-c-12-phac-act/
(17) https://www.qp.alberta.ca/documents/Acts/P37.pdf
(18) https://www.facebook.com/kenneyjasont/videos/1065515287297927