

It was recently revealed that the Justice who presided over several anti-lockdown cases in British Columbia runs a group called the Vancouver Foundation. Looking into the details of this charity a bit more, this creates — at a minimum — the appearance of a potential conflict of interest. (See archive.)
The group describes itself in this way:
“Vancouver Foundation grants to hundreds of charities and non-profits in BC every year. Our vision is to create healthy, vibrant, and livable communities, and we focus on supporting projects that address the root causes of important issues. Our funding comes from generous gifts from the community, as well as from managing endowment funds for people, charities, and businesses.”
The Vancouver Foundation is involved in many different areas, and has undoubtedly has done a lot of good work. However, some things need to be questioned.
Anyhow, this is quite the rabbit hole, so let’s jump in.
The Vancouver Foundation Act is what governs the organization. This isn’t a traditional group, but one that was created in 1943 by an Act of Parliament.
Board of directors
5 (1) The board of directors of the foundation is to consist of at least 10 and not more than 18 persons, with the directors determining the number of directors from time to time in the bylaws of the foundation.
(1.1) If the number of directors is below the minimum number set out in subsection (1) or in the bylaws, as applicable, the board continues to have the authority to carry out its duties and exercise its powers until all vacancies are filled.
(1.2) Subject to section 6, the board consists of the following members:
(a) the Chief Justice of the Supreme Court of British Columbia or, if applicable, the judge appointed by the Chief Justice under that section;
(b) a member of the Law Society of British Columbia who has been nominated by the Law Society of British Columbia in accordance with the bylaws of the foundation and whose nomination has been accepted by the board;
Chief Justice Christopher Hinkson is a Director at the Vancouver Foundation, by virtue of his position on the Court. Far from being just a name on paper, he’s prominently listed as a Director (see margin on page 3). He also made the following rulings:
COURT CASES PRESIDED OVER BY CHIEF JUSTICE HINKSON
(A) Kassian v. British Columbia, 2022 BCSC 1603
(Refusal for exemption to vaccine passport)
https://www.canlii.org/en/bc/bcsc/doc/2022/2022bcsc1603/2022bcsc1603.html
(B) Eliason v. British Columbia (Attorney General), 2022 BCSC 1604
(Refusal for charter rights to travel, s.6 of Charter)
https://www.canlii.org/en/bc/bcsc/doc/2022/2022bcsc1604/2022bcsc1604.html
(C) Maddock v. British Columbia, 2022 BCSC 1605
(Refusal for compensation due to injury)
https://www.canlii.org/en/bc/bcsc/doc/2022/2022bcsc1605/2022bcsc1605.html
(D) CSASPP v. British Columbia, 2022 BCSC 1606
(Refusal to allow health care workers to opt out)
https://www.canlii.org/en/bc/bcsc/doc/2022/2022bcsc1606/2022bcsc1606.html
(E) Beaudoin v. British Columbia, 2021 BCSC 248, BCSC 248
(Refusal to allow a church to remain open)
https://www.canlii.org/en/bc/bcsc/doc/2021/2021bcsc512/2021bcsc512.html
True, one might get the impression that he simply called these cases as he saw fit. But there is more to things than meet the eye.
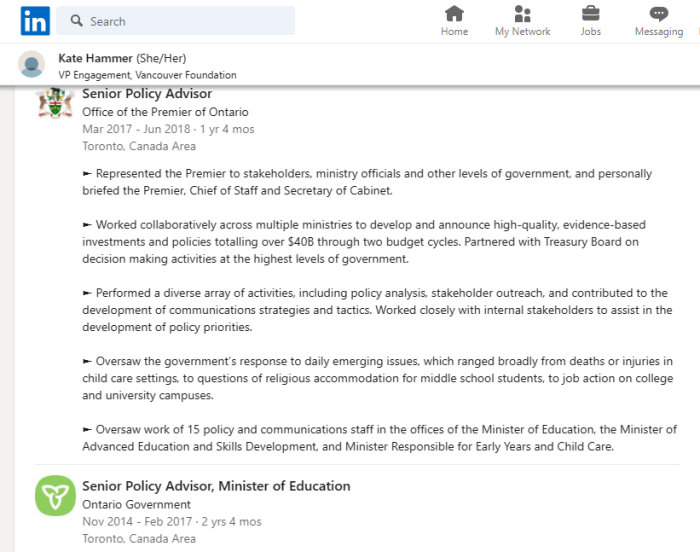
Kate Hammer is the Vice President for Engagement, was previously a Senior Policy Advisor for the Minister of Education (Ontario), and also worked in the Office of the Premier under Kathleen Wynne. Sure, that’s Ontario, but people in political circles have very deep networks of connections, and it’s rarely limited to a region. (See archive.)
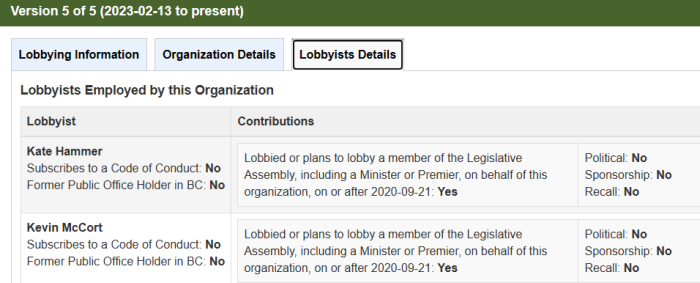
She’s also now lobbying the B.C Government on behalf of the Vancouver Foundation. Things get even more convoluted. Why? Because the B.C. Lobbying Registry shows exactly what subject matters are being discussed.
The Vancouver Foundation is trying to get more access and influence from the B.C. Government. This can cause a problem.
- Activities to support an amendment to Vancouver Foundation Act related to definition of “reserve amount”
- Vancouver Foundation seeks to discuss with the BC Government options and opportunities for ensuring legislation and regulations related to lobbyists transparency do not limit charities and non-profits from participating in vital conversations about government policies and priorities.
- Vancouver Foundation seeks to discuss with the BC Government options and opportunities for the charitable sector to play a key role in pandemic recovery
- Vancouver Foundation seeks to discuss with the BC Government options for expanding the Unclaimed Property Act’s ability to use dormant assets to boost investment in community initiatives and organizations.
Let’s think about this one. Chief Justice Hinkson, a Director at the Vancouver Foundation, is making key Court rulings relating to “pandemic measures”. Meanwhile, his organization is lobbying the B.C. Government for greater influence in exactly those areas.
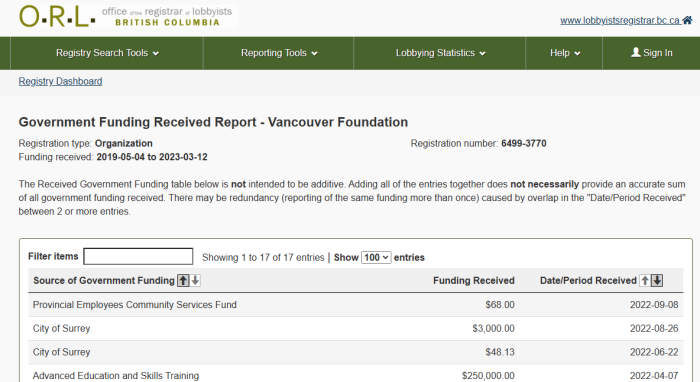
And what taxpayer sources is the Vancouver Foundation getting money from?
| SOURCE | DATE | AMOUNT |
|---|---|---|
| Provincial Employees Community Services Fund | 2022-09-08 | $68.00 |
| City of Surrey | 2022-08-26 | $3,000.00 |
| City of Surrey | 2022-06-22 | $48.13 |
| Advanced Education and Skills Training | 2022-04-07 | $250,000.00 |
| Children and Family Development | 2022-04-05 | $2,760,000.00 |
| Social Development and Poverty Reduction | 2022-04-01 | $1,350,000.00 |
| Social Development and Poverty Reduction | 2022-04-01 | $30,000,000.00 |
| Canada Cultural Investment Fund | 2022-03-21 | $1,005,258.00 |
| City of Vancouver | 2022-03-11 | $45,000.00 |
| Forests, Lands, Natural Resource Operations, and Rural Development | 2022-02-24 | $5,000,000.00 |
| City of Surrey | 2020-10-08 | $45.00 |
| BC Arts Council | 2020-04-02 | $200,000.00 |
| Social Development and Poverty Reduction | 2020-04-02 | $590,000.00 |
| Advanced Education, Skills and Training | 2020-03-31 | $250,000.00 |
| Canada Cultural Investment Fund | 2020-03-16 | $955,718.00 |
| Provincial Employees Community Services Fund | 2020-03-13 to 2020-09-10 | $59.80 |
| City of Vancouver | 2020-03-13 | $22,500.00 |
The Vancouver Foundation has received several millions of taxpayer money in the last few years.
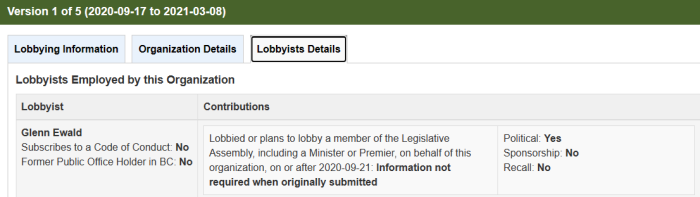
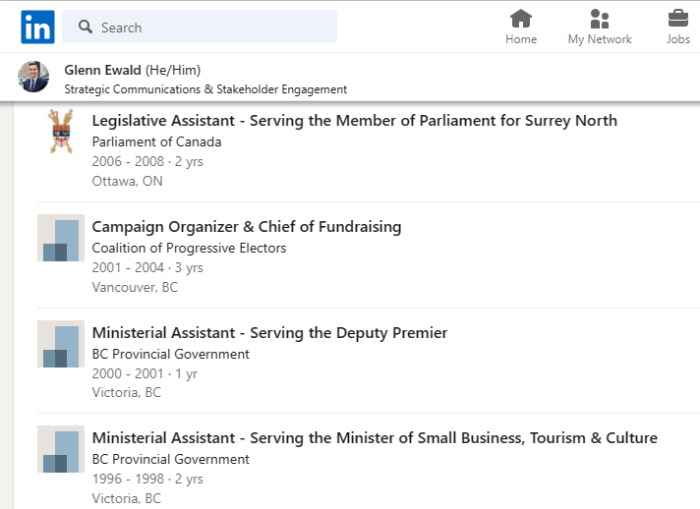
Glenn Wald gets an honourable mention. He was the Director of Communications at Vancouver Foundation from November 2017 until October 2022. He has also been involved with both the Federal and British Columbia Governments. (See archive.)
Joe Gallagher, Vice President Indigenous Health & Cultural Safety at Provincial Health Services Authority, is also worth listing. He was a Board Member at the Vancouver Foundation until July 2022, so very recent. (See archive.)
Dara Parker is formerly a Program Manager for the United Nations Association in Canada, and an advisor for the U.N. Human Resettlements Programme. (See archive.)
As covered previously, the B.C. Centre for Disease Control (BCCDC) Foundation is in fact a registered charity that contributes substantial amounts annually to up to 4 “qualified donees”. These are:
- B.C. Centre for Disease Control
- Community-Based Research Centre Society (also a charity)
- Provincial Health Services Authority (also a charity)
- University of British Columbia (also a charity)
The BCCDC Foundation used to have a scroller to cycle through their major donor list. It’s since been removed, but thankfully saved in an earlier article:
The BCCDC Foundation proudly lists the Vancouver Foundation as a donor, as well as companies like Pfizer. The BCCDC-F also admits that a significant portion of its funding comes from pharmaceutical companies. Is it any wonder why the B.C. Government is so pro-pharma?
In terms of following the money, the next sections are from CSASPP’s March 12, 2023 summary for the Vancouver Foundation’s financials. As a registered charity, it’s required to disclose a fair amount of information publicly. Rather than reinvent the wheel, here are the highlights:
Based on the T3010 Registered Charity Information Return filed with the Canada Revenue Agency, several years of reporting periods are available. The records are copious with thousands of donees. We will save you the trouble of sifting through them. The following is a summary of our provisional material findings.
In fiscal year 2021 the Vancouver Foundation donated to the Public Health Association of British Columbia $193,072 and to Fraser Health Authority $93,434. The year prior of 2020 Vancouver Coastal Health Authority received $100,000 from the Foundation. A charity setup by the British Columbia Centre for Disease Control to receive donations, the BCCDC Foundation for Population and Public Health, received $13,000.
During the onset to the alleged pandemic in 2019, many of you will recall the traditional intellectual safeguards were largely mute. The British Columbia Civil Liberties Association received $151,718.
Other recipients during that fiscal year include the BCCDC’s Foundation at $57,667, Fraser Health Authority at $41,055, the Registered Nurses Foundation of BC at $4,276, and a charity setup by the Canadian Broadcasting Corporation at a $1,000.
The previous fiscal year of 2018 the BCCDC Foundation again received $57,667, Fraser Health Authority $41,472, the BC Civil Liberties Association $36,104, and the CBC’s charity $1,000.
From the voluminous records we were able to analyze in the time invested, this is where money directly went. The question of where money went after the Vancouver Foundation donated it to the BCCDC Foundation is also worth commenting on.
Unlike the Vancouver Foundation, the BCCDC’s Foundation does not donate to thousands of donees. Based on its own T3010 filing, from fiscal years 2017 to 2021, it donates to only one to four donees a year. A sophisticated organization, such as the Vancouver Foundation, cannot reasonably be said to not know where the aforementioned benefactor receiving a donation would subsequently direct it to.
In every filing we uncovered problematic benefactors. In fiscal year 2021 the BCCDC Foundation donated to the Provincial Health Services Authority $140,247. The year prior of 2020 an amount of $487,689 was donated to the PHSA. In 2019 they received $588,553. In 2018 they received $290,267. In 2017 they received $426,016. The BCCDC Foundation then in 2017 donated to the BCCDC itself $15,300.
Recall that the PHSA is Dr. Henry’s employer, a defendant named in all of our litigation – including the petition in which the Chief Justice presided over. It is impossible for any reasonable person to characterize the movement of substantial sums of money in this manner under the direction of the Chief Justice as, at the very least, not carrying the perception of a conflict of interest.
What is the result of all of this? We get a situation where there really is no separation between the judiciary, the legislature, and N.G.O.s with financial interests. Everything seems to blend together.
Was there anything to those anti-lockdown rulings in B.C.? Impossible to say for sure, but the connections of the Vancouver Foundation do raise a lot of questions.
SOURCES:
(1) https://www.vancouverfoundation.ca/detail/chief-justice-christopher-hinkson/
(2) https://archive.is/wPjZm
(3) https://www.bclaws.gov.bc.ca/civix/document/id/lc/psl/00032_01
(4) https://www.vancouverfoundation.ca/about-us/our-people/our-team/
(5) http://2007.vancouverfoundationvitalsigns.ca/sites/default/files/publications/VF_Magazine_2020_web.pdf
(6) https://www.lobbyistsregistrar.bc.ca/app/secure/orl/lrs/do/vwRg?cno=3770®Id=56555677
(7) https://www.lobbyistsregistrar.bc.ca/app/secure/orl/lrs/do/reports/funding/received?cocId=3770®Id=56555677&extnl=true
(8) https://www.lobbyistsregistrar.bc.ca/app/secure/orl/lrs/do/vwRg?cno=3770®Id=56567332
(9) https://www.linkedin.com/in/kate-hammer-5226a6a6
(10) https://archive.is/9RHmI
(11) https://www.linkedin.com/in/daraparker/details/experience/
(12) https://archive.is/cNFEY
(13) https://www.linkedin.com/in/glennewald/details/experience/
(14) https://archive.is/QFi7M
(15) https://www.linkedin.com/in/joe-gallagher-1730a0b3/
(16) https://archive.is/SL24p
(17) https://www.covidconstitutionalchallengebc.ca/status-updates
(A) BCCDC Foundation Charity Page
(B) University Of British Columbia Charity Page
(C) Provincial Health Services Authority Charity Page
(D) Community-Based Research Centre Society Charity Page
(E) Vancouver Foundation Charity Page