
The work that real truthers do is invaluable. As an example, there are many, like Fluoride Free Peel, proving this “deadly virus” doesn’t really exist. Another one to look up is Andrew Kaufman.
Under the quack definition of “isolation”, alleged viruses are supposedly isolated by mixing them with bovine, pig or monkey cells and cultured. An obvious question would be: why aren’t samples taken directly from the patient? It would be comical if not for the fact that a lot of people take this seriously.
For those not wishing to get involved in a scientific debate, let’s do something simpler. What exactly is a Covid death, according to the World Health Organization? What strict scientific and medical standards are applied in making such diagnoses?
We are always told to trust the science. But what do the official guidelines say about what a “Covid death” really is?
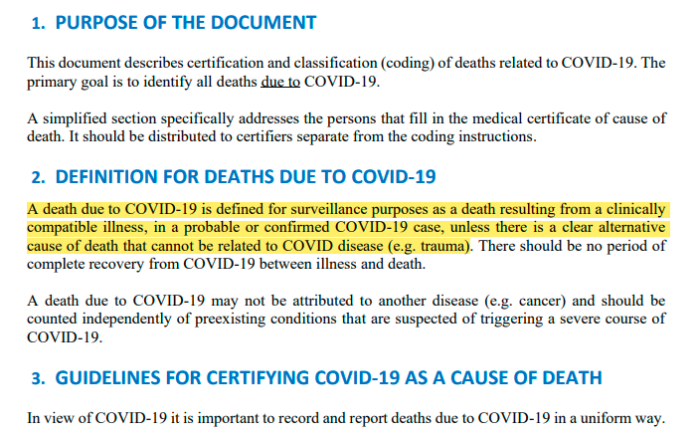
2. DEFINITION FOR DEATHS DUE TO COVID-19
A death due to COVID-19 is defined for surveillance purposes as a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma). There should be no period of complete recovery from COVID-19 between illness and death.
.
A death due to COVID-19 may not be attributed to another disease (e.g. cancer) and should be counted independently of preexisting conditions that are suspected of triggering a severe course of COVID-19.
Unfortunately, this isn’t satire. The WHO actually provides this incredibly vague and meaningless definition. (See archive here). It’s been covered elsewhere on this site, but so far, hasn’t had an article devoted to it.
Not only is there the issue of no isolation, WHO recommends in its March 2020 (see page 3), and September 2020 (see page 8), guidance NOT to isolate for routine testing.
Perhaps WHO just doesn’t want proper testing done normally to save money?! Well, not really, their own paperwork (see archive) indicates that they view testing for just a gene to be sufficient.
If the included video isn’t of high enough resolution (it was compressed), then it’s available on Odysee or Bitchute as well.
There are plenty of other examples of this. Please, do a little digging, using the definition provided above. The above video contains several cases of this fraudulent definition being used, but many more are available.
(1) https://www.who.int/classifications/icd/Guidelines_Cause_of_Death_COVID-19.pdf
(2) WHO Guidelines Classification Of Death
(3) https://www.bitchute.com/video/iKXqxr8RgNQz/
(4) https://odysee.com/@CanuckLaw:8/Definitions-Matter:d
(5) https://www.fluoridefreepeel.ca/fois-reveal-that-health-science-institutions-around-the-world-have-no-record-of-sars-cov-2-isolation-purification/
(6) https://canucklaw.ca/wp-content/uploads/2021/01/WHO-COVID-19-laboratory-Testing-March-17-2020.pdf
(7) https://canucklaw.ca/wp-content/uploads/2021/01/WHO-2019-nCoV-laboratory-September-11-2020-Guidelines.pdf