

The World Health Organization Constitution is just one document that Canadians were subjected to, and this being done without knowledge or consent. Was there ever a referendum or election campaign run on this? Probably not.
The full text is available with a quick internet search. Below are some sections which might be the most troubling to any nationalist or patriot.
Article 4
Members of the United Nations may become Members of the Organization by signing or otherwise accepting this Constitution in accordance with the provisions of Chapter XIX and in accordance with their constitutional processes.
This part cannot be overemphasized. If a country wants to be part of the WHO, then they necessarily have to sign onto their constitution. The Federal Government did this on their own, with a signature. And as we go through it, the problems with this become obvious.
Article 7
If a Member fails to meet its financial obligations to the Organization or in other exceptional circumstances, the Health Assembly may, on such conditions as it thinks proper, suspend the voting privileges and services to which a Member is entitled. The Health Assembly shall have the authority to restore such voting privileges and services.
So, being part of this group is voluntary. However, if you don’t pay your bills, WHO can suspend your voting rights. They can also be removed under the undefined “exceptional circumstances”. Sounds a bit undemocratic, doesn’t it?
Article 19
The Health Assembly shall have authority to adopt conventions or agreements with respect to any matter within the competence of the Organization. A two-thirds vote of the Health Assembly shall be required for the adoption of such conventions or agreements, which shall come into force for each Member when accepted by it in accordance with its constitutional processes.
Article 20
Each Member undertakes that it will, within eighteen months after the adoption by the Health Assembly of a convention or agreement, take action relative to the acceptance of such convention or agreement. Each Member shall notify the Director-General of the action taken, and if it does not accept such convention or agreement within the time limit, it will furnish a statement of the reasons for non-acceptance. In case of acceptance, each Member agrees to make an annual report to the Director-General in accordance with Chapter XIV
The Health Assembly has the right to determine its own conventions and agreement, and it can be done with a 2/3 vote. By this rationale, Canada could easily be forced into adopting policies that it fundamentally disagrees with. And to state the obvious, there was never any domestic vote or referendum over this.
Members are also obligated to go along with any convention or agreement. If they refuse, written reasons have to be provided.
Article 21
The Health Assembly shall have authority to adopt regulations concerning:
(a) sanitary and quarantine requirements and other procedures designed to prevent the international spread of disease;
(b) nomenclatures with respect to diseases, causes of death and public health practices;
(c) standards with respect to diagnostic procedures for international use;
(d) standards with respect to the safety, purity and potency of biological, pharmaceutical and similar products moving in international commerce;
(e) advertising and labelling of biological, pharmaceutical and similar products moving in international commerce.
Article 22
Regulations adopted pursuant to Article 21 shall come into force for all Members after due notice has been given of their adoption by the Health Assembly except for such Members as may notify the Director-General of rejection or reservations within the period stated in the notice.
W.H.O.’s constitution makes it clear that quarantine measures fall under their purview. Quarantine, of course, is code for movement and population control. Strange how none of the freedom fighters in the media or politics ever mention this.
As for the standards and nomenclature of pharmaceuticals, this includes vaccines that are pushed on the public despite only having emergency authorization. There’s also a reference to testing, such as the PCR tests, which can’t determine anything.
W.H.O. names diseases as well, including ones that have never been proven to exist.
It doesn’t appear that Canada ever rejected or opted-out of any of this. As such, we are compelled to play along with this globalist organization.
Article 54
The Pan American Sanitary Organization represented by the Pan American Sanitary Bureau and the Pan American Sanitary Conferences, and all other inter-governmental regional health organizations in existence prior to the date of signature of this Constitution, shall in due course be integrated with the Organization. This integration shall be effected as soon as practicable through common action based on mutual consent of the competent authorities expressed through the organizations concerned.
All other organizations that use “public health” as a means of population control will eventually become integrated with W.H.O. Guess it keeps everything centralized.
CHAPTER XIII – VOTING
Article 59
Each Member shall have one vote in the Health Assembly.
Article 60
(a) Decisions of the Health Assembly on important questions shall be made by a two-thirds majority of the Members present and voting. These questions shall include: the adoption of conventions or agreements; the approval of agreements bringing the Organization into relation with the United Nations and inter-governmental organizations and agencies in accordance with Articles 69, 70 and 72; amendments to this Constitution.
(b) Decisions on other questions, including the determination of additional categories of questions to be decided by a two-thirds majority, shall be made by a majority of the Members present and voting.
(c) Voting on analogous matters in the Board and in committees of the Organization shall be made in accordance with paragraphs (a) and (b) of this Article.
This becomes a numbers game, where decisions that are detrimental to some nations can be adopted simply because the majority overall vote for it. With this mechanism in mind, there really is no sovereignty to rely on.
CHAPTER XV – LEGAL CAPACITY, PRIVILEGES AND IMMUNITIES
Article 66
The Organization shall enjoy in the territory of each Member such legal capacity as may be necessary for the fulfilment of its objective and for the exercise of its functions.
Article 67
(a) The Organization shall enjoy in the territory of each Member such privileges and immunities as may be necessary for the fulfilment of its objective and for the exercise of its functions.
(b) Representatives of Members, persons designated to serve on the Board and technical and administrative personnel of the Organization shall similarly enjoy such privileges and immunities as are necessary for the independent exercise of their functions in connexion with the Organization.
Article 68
Such legal capacity, privileges and immunities shall be defined in a separate agreement to be prepared by the Organization in consultation with the Secretary-General of the United Nations and concluded between the Members
All employees and other workers are given immunity from legal action as part of their contracts with W.H.O. That’s a pretty good deal. They can’t be sued, charged, or have recourse taken against them, as long as they were doing their jobs. There doesn’t even seem to be a requirement that they be acting in good faith.
Article 69
The Organization shall be brought into relation with the United Nations as one of the specialized agencies referred to in Article 57 of the Charter of the United Nations. The agreement or agreements bringing the Organization into relation with the United Nations shall be subject to approval by a two-thirds vote of the Health Assembly.
The W.H.O. would be subject to U.N. control. It’s pretty clear that the ultimate goal is to merge all of these organizations into a single, centralized institution of power.
Article 71
The Organization may, on matters within its competence, make suitable arrangements for consultation and co-operation with non-governmental international organizations and, with the consent of the Government concerned, with national organizations, governmental or non-governmental
On its own, this doesn’t sound too bad, but the devil is always in the details. Which groups would be consulted? How would they be screened? Would their recommendations become binding on members?
Article 72
Subject to the approval by a two-thirds vote of the Health Assembly, the Organization may take over from any other international organization or agency whose purpose and activities lie within the field of competence of the Organization such functions, resources and obligations as may be conferred upon the Organization by international agreement or by mutually acceptable arrangements entered into between the competent authorities of the respective organizations.
The W.H.O. constitution gives itself the power to take over from any “international organization or agency” within its designated scope, as long as there is a 2/3 majority vote from the Health Assembly.
Sure, it’s done “on consent”, but who are the people that are really consenting?
Article 79
(a) States may become parties to this Constitution by:
(i) signature without reservation as to approval;
(ii) signature subject to approval followed by acceptance; or
(iii) acceptance.
(b) Acceptance shall be effected by the deposit of a formal instrument with the Secretary-General of the United Nations.
Article 80
This Constitution shall come into force when twenty-six Members of the United Nations have become parties to it in accordance with the provisions of Article 79.
This isn’t everything, but just more eye-opening parts. The full text of the W.H.O. constitution is freely available. (Here’s the highlighted version). Look it up, read it, and see what exactly we have been signed onto without any sort of democratic mandate.
Rest assured, there are a lot more than 26 countries now. This means the constitution has come into force. And if anyone hasn’t gone through the chronology of events, it’s all laid out here:
1908: International Public Health Office to be created
1926: International Sanitary Convention was ratified in Paris.
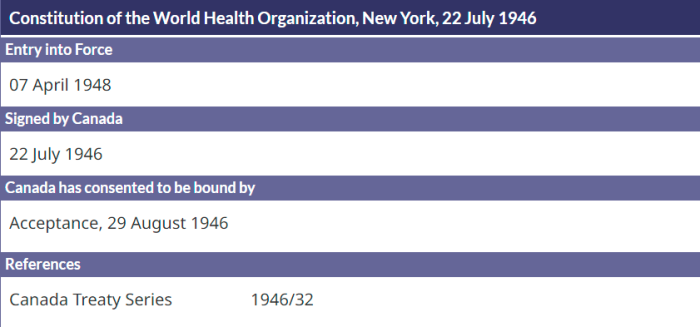
1946: WHO’s Constitution was signed, and it’s something we’ll get into in more detail.
1951: International Sanitary Regulations adopted by Member States.
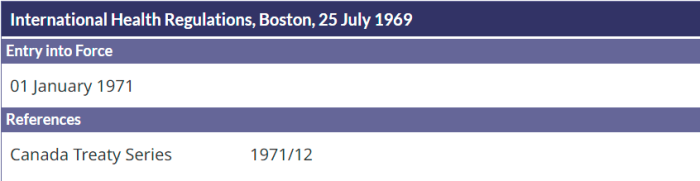
1969: International Health Regulations (1st Edition) replaced ISR. These are legally binding on all Member States.
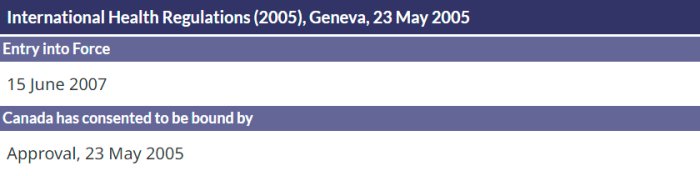
2005: International Health Regulations 3rd Edition of IHR were ratified.
Being part of the World Health Organization means submitting to their rules and control. It’s laid out in their own constitution. To be clear, sovereignty will never be possible as long as Canada is part of this entity.
As has been outlined here before, the 2005 Quarantine Act, Bill C-12, was really just domestic implementation of the 3rd Edition of the International Health Regulations.
We’ve also gone heavily into the creation of PHAC, which is essentially just a branch of the World Health Organization. It was created at WHO’s instigation. It takes over (to a large degree) what Health Canada had been doing. The timeline is laid out, and worth a read.
The W.H.O. Constitution is a major step is the erasure of nations — under the guise of public health. Anyone serious about “freedom” in Canada, or elsewhere, needs to address this. Far too many are propped up as heroes, but who ignore the underlying legislation and treaties.
(1A) https://canucklaw.ca/wp-content/uploads/WHO-Constitution-Full-Document.pdf
(1B) WHO Constitution Full Document MARKED
(2) https://www.who.int/about/governance/constitution
(3) https://apps.who.int/gb/bd/
(4) https://apps.who.int/gb/bd/pdf_files/BD_49th-en.pdf#page=6
(5) https://www.treaty-accord.gc.ca/
(6) https://www.treaty-accord.gc.ca/index.aspx
(7) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=103984&t=637793587893732877
(8) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=103986&t=637862410289812632
(9) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=103990&t=637793587893576566
(10) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=103994&t=637862410289656362
(11) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=103997&t=637793622744842730
(12) https://www.treaty-accord.gc.ca/details.aspx?lang=eng&id=105025&t=637793622744842730