
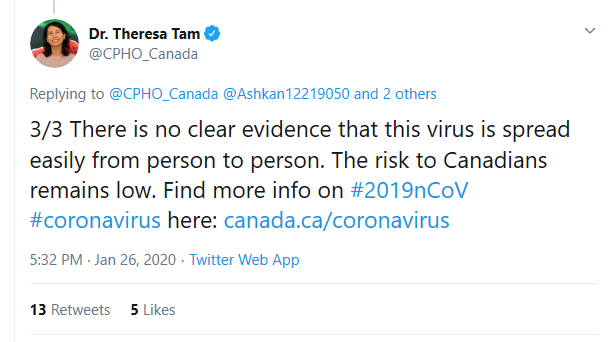
As of late January, 2020, Theresa Tam saw very little risk to Canadians, and that human to human transmission was not a threat
1. Other Articles On CV “Planned-emic”
The rest of the series is here. Many lies, lobbying, conflicts of interest, and various globalist agendas operating behind the scenes. The Gates Foundation finances: the World Health Organization, the Center for Disease Control, GAVI, ID2020, John Hopkins University, Imperial College London, the Pirbright Institute, the British Broadcasting Corporation, and individual pharmaceutical companies. Also: there is little to no science behind what our officials are doing; they promote degenerate behaviour; the Australian Department of Health admits the PCR tests don’t work; the US CDC admits testing is heavily flawed; and The International Health Regulations are legally binding. See here, here, and here.
2. Important Links
(1) https://twitter.com/i/status/1221242779923374081</a
(2) https://en.wikipedia.org/wiki/Theresa_Tam
(3) http://archive.is/e9jwT
(4) Translated Article
(5) https://www.longwoods.com/articles/images/Canada_Pandemic_Influenza.pdf
(6)Tam.Canada_Pandemic_Influenza.2006.report
(7) https://www.theglobeandmail.com/canada/article-ottawa-had-a-playbook-for-a-coronavirus-like-pandemic-14-years-ago/
(8) http://archive.is/oBxhf
3. Is Theresa Tam Really Tan Yongshi?


Also check out this link, from an article that identifies Tam as “Tan Yongshi”. Credit is due to Christina Forbes for catching this is the first place.
As the chief health officer, what are the negligent duties that Ms. Tan Yongshi should step down from? In general, there are five aspects. First of all: she should be vigilant about the lack of the new crown epidemic. Wuhan was closed on January 23, and the first patient appeared in Canada on January 25. On January 30, WHO declared the new coronary pneumonia as a public health emergency, and the United States announced the closure of China the next day. At that time, the Chinese community understood the seriousness of the virus and appealed to the government to be vigilant, but Tan was indifferent to it and repeatedly emphasized that Canada’s risk was very low, thus missing the best time for prevention and control. After the closure of the United States, because Canada did not take measures, many travelers detoured to Canada to the United States. During their stay in Canada, they planted hidden dangers for the spread of the virus.
Second: Due to the contempt of Tan Yongshi and the government, the Canadian border epidemic prevention and isolation measures are useless. Among the countries in the world, Canada is the only country that has no airport temperature measurement since the outbreak. In the early stage of the epidemic, all entrants were only verbally asked whether they came from the epidemic area, and there was no requirement for isolation. Nevertheless, most Chinese are consciously isolated for 14 days. In the middle of the outbreak, although the government made a 14-day quarantine request, there was no compulsory follow-up measure. Now that the epidemic has almost peaked, the government has proposed coercive measures, but there is no guarantee of law enforcement, because the RCMP responsible for law enforcement has not issued a ticket. If it is said that Trudeau did this based on Ms. Tan ’s opinion, then Tan did not warn against the strengthening of airport detection and isolation, which is her negligence.
There appear to be translation issues, as it switches names several times. Nonetheless, it does refer to Theresa Tam as Tan Yongshi.
It would be nice to nail this down for certain. Should any reader come across this and have more information, please share. Personally, it would be nice to have more material than: (1) a Wikipedia page; and (2) an article from Google Translate.
To play some devil’s advocate, even if this is the case, it may be attempt to simply adopt a more English sounding name. Many people have done it before.
4. Critique Of 2006 Epidemic Plan
A 2006 report co-written by Dr. Theresa Tam – now the face of Canada’s COVID-19 response – predicted our current situation, and the steps needed to get out of it, with eerie accuracy. But the actual response has been very different
A pandemic sweeps across Canada in one or two months. It is spread not only by the sick, but by people who show no symptoms. There are shortages of medical supplies and the health system struggles to keep up. The peak won’t come for months, and it will be accompanied by a surge in deaths. Soon after, the country will brace for a second wave.
All of this is now true for the COVID-19 crisis, but the aforementioned scenario – a warning – comes from a 2006 federal report on pandemic preparedness. Fourteen years later, its words are eerily accurate.
Despite the prescience of such warnings, Canada and many other governments around the world significantly underestimated the severity of the coronavirus.
As recently as late January, federal officials, including Dr. Tam, said the threat of a major outbreak in Canada was very low, that measures such as travel restrictions weren’t needed, and that the risk of the virus being spread by people without symptoms was highly unlikely.
The article goes on to criticize the Federal Government’s lack of preparedness in many different ways, and in great detail. To their credit, the Globe & Mail is pretty thorough in many ways.
But what they missed in their critique is the propaganda elements within the 2006 report. They may be subtle, but they are there.
5. Contents Of 2006 Report
For vaccine program planning purposes, it is important to be prepared to immunize 100% of the population; however, the actual proportion of the population that will voluntarily seek vaccination will depend on public perception of the risk and the severity of the disease. Therefore, the demand, which will manifest as clinic attendance, will likely vary among jurisdictions and within each jurisdiction as the pandemic evolves. Previous experience with outbreak-related immunization clinics indicates that it would be prudent to prepare for an initial demand of 75% of the target population. It is recommended that planning activities also focus on delivering a two dose program to ensure that the public health response is ready to deal with this possibility.
Tam.Canada_Pandemic_Influenza.2006.report
If you go to section 2.2 (page 60 in the 550 page pdf file), it does point out an interesting fact: that the amount of people who will voluntarily take a vaccination depends on the public perception of risk.
Therefore: one can reasonably conclude from this, if the goal is mass vaccination of the public, it is necessary to get them afraid, and keep them afraid.
The Canadian Pandemic Influenza Plan for the Health Sector (the Plan) consists of an introduction and a background section, followed by the preparedness, response and recovery sections, which are consistent with the general principals of emergency response. Each section aims to assist and facilitate appropriate planning for the health sector at all levels of government for the next influenza pandemic. The Plan and the annexed guidelines, checklists and other documents were developed to assist all jurisdictions with the main components of health sector planning, including surveillance, vaccine programs, use of antivirals, health services, public health measures and communications. The most effective public health intervention to mitigate the impact of a pandemic is through immunization with an effective vaccine against the novel virus, and, to a lesser extent, through the use of antiviral drugs. In addition, comprehensive planning requires that appropriate surveillance capacity is in place, and that the health sector, emergency services and communities as a whole are informed and equipped to deal with a pandemic.
This is from the PREFACE (page 21 in 550 page pdf file). It states that the best solution is a vaccine against the novel virus, and that antivirals are a lesser option. Okay, so every time there is a “novel” virus, we need to break out the vaccine testing?
The preface also states that an appropriate surveillance capacity is needed. Perhaps it could be forcing people to wear bracelets, as Theresa Tam/Tan Yongshi suggests.
The components of the 2004 edition of the Plan included surveillance, vaccine programs, antivirals, health services, emergency services, public health measures and communications. In this edition of the Plan, the emergency services component has been removed; it is now addressed as part of the preparedness for overall emergency management and coordination.
Federal, provincial, territorial and local planners are encouraged to consider the psychosocial implications of pandemic influenza when developing their plans for preparedness and response activities. It is anticipated that a component focusing on psychosocial issues will be added to future versions of the Plan.
Section 2.0 (page 54 of the 550 page pdf) openly states that surveillance and vaccine programs are to be prominent portions of this plan. It seems nothing has changed.
Jurisdictions need to be prepared to rapidly implement or modify enhanced surveillance activities. For the purpose of informing public health risk assessment and response activities, a coordinated and rapid epidemiological investigation that includes the collection, collation and analysis of detailed epidemiological, laboratory and clinical data is required. Further, rapid sharing of data and efficient communication at all levels of government are critical for facilitating a coordinated response.
At the federal level, regular environmental scanning for the detection of potentially significant ILI is conducted using official information sources for influenza surveillance (e.g. World Health Organization [WHO] and government influenza surveillance programs from other countries) and unconfirmed reports from early warning systems (e.g. ProMed and other media scanning software, such as the Global Public Health Intelligence Network).
On an ongoing basis, the newly created national expert Working Group for Vaccine Preventable and Respiratory Infections Surveillance (VPRIS-N) will be assessing surveillance systems and making recommendations for enhancements and improvements for the Interpandemic, Pandemic Alert and Pandemic Periods. Recommendations from this group are being refined on an ongoing basis; current recommendations are included in Annex N, Pandemic Influenza Surveillance Guidelines.
The report in this focuses on the need for new surveillance methods (page 56 of 550 page pdf). While avoiding specifics, it acknowledges that expanding it would be greatly beneficial.
Because surveillance data will drive the pandemic response, it is important that physicians and other health care workers are educated and updated on an ongoing basis about the importance of ILI surveillance as well as their roles in the system. Surveillance systems must be established in advance of a pandemic because there will be little time to augment capacity at the time of a pandemic. At the time of a pandemic, surveillance and laboratory-testing capacity will be reduced (e.g. due to staff absenteeism and potential supply shortages) compared with pre-pandemic periods; only streamlined, resource-efficient systems will continue to function. Special study protocols if required (e.g. to determine epidemiology or to investigate reported adverse events following immunization) at the time of a pandemic must be developed and pretested during the pre-pandemic period, recognizing that refinements may be necessary at the time of a pandemic.
However, on the next page, the report suggests that surveillance systems must be established well in advance, as it may not be possible later. Again, avoiding specifics about what that surveillance would be about?
Vaccination of susceptible individuals is the primary means to prevent disease and death from influenza during an epidemic or pandemic. The National Advisory Committee on Immunization (NACI) produces annual recommendations on the use of influenza vaccine in persons who are most at risk for influenza or those who could spread influenza to persons at greatest risk. These interpandemic recommendations are published annually in the Canada Communicable Disease Report. In the event of a pandemic, PIC, which includes representation from NACI, will provide recommendations to F/P/T immunization programs on the development, production and use of the pandemic vaccine, and priority groups for immunization. Efforts should be made to encourage all jurisdictions to adopt the national recommendations on priority groups at the time of a pandemic in order to facilitate equitable access and consistent messaging.
That’s from page 57. “Consistent messaging”??? Does that mean that government officials should keep their talking points consistent in order to prevent the public from picking out contradictions?
From page 59 of the report. In case you were wondering “recombinant vaccines” are ones that are made up of combined genetic material. Think of it as a Franken-vaxx.
Vaccines, when available, will be the primary public health intervention during a pandemic. However at the start of the pandemic, vaccines may not be available as soon as required and two doses of vaccine may be necessary to achieve an adequate immune response. Antivirals (anti-influenza drugs) are effective for both treatment and prophylaxis of annual influenza. These drugs were not available during past pandemics, but are expected to be effective against pandemic strains of the influenza virus. Antivirals will likely be the only virus-specific intervention during the initial pandemic response. Protection afforded by antivirals is virtually immediate and does not interfere with the response to inactivated influenza vaccines.
From page 61. Vaccines are to be the primary defence against an outbreak.
During a pandemic, antiviral strategies should use all the types of effective anti-influenza drugs that are available to Canadians, and should be adaptable to changing disease epidemiology and vaccine availability. If the novel virus is found to be susceptible to amantadine, which is not currently part of the National Antiviral Stockpile, it is recommended that amantadine be used for prophylaxis (not treatment) only. Oseltamivir could be used for both treatment of cases and prophylaxis. The efficacy of oseltamivir and amantadine are approximately equal for the treatment of cases infected with sensitive strains; however, amantadine is recommended exclusively for prophylaxis to minimize the development of amantadine resistance (which would render the drug ineffective) during the pandemic. The timing of the use of antivirals during a pandemic should be guided by local surveillance data.
From page 63. We think antivirals are okay, but only as long as they don’t interfere with vaccines at some point in the future.
This 550 page report is too long to go through in a single article. However, it’s morbid how much: (a) surveillance; and (b) vaccines are woven into the entire report. It reads as if the entire research was to set up a police state and drug everyone.
The Globe & Mail article referenced in the last section complained that the Federal Government was grossly unprepared considering this 2006 report. While true in some sense, the G&M authors apparently didn’t bother to actually read this report before publishing their article.
6. Vaxx/Surveillance Planned From 2004?
How long exactly has this been going on for? How long has this plan been in the works for? It can’t just be a series of random and unrelated events. Has it been going on for much longer that 16 years?
- In 2004, this research begins.
- In 2006, it is released. It recommends heavy surveillance, and vaccinations for everyone.
- In 2010, Theresa Tam/Tan Yongshi participated in the film “Outbreak Of An Epidemic”, which depicted a fictional simulation of the Federal Government responding to a pandemic.
- In 2017, Raj Saini (who is pharma lobbied), introduced M-132, to fund drug research and get drugs out to Canadians, and to the world at large.
- In October 2019. Event 201 took place. This was the Gates-involved simulation which would see tens of millions of people die in a computer model of an outbreak.
Again, credit to Civilian Intelligence Network for digging up the 2010 film. The whole thing reads like a giant dress rehearsal for the actual shut down.
An interesting observation in the report: voluntary vaccinations will happen in much larger numbers if people feel the threat is real and imminent. That may explain all the dire warnings coming from the government.
As for Theresa Tam, is that her real name? To be fair, even if true, it could be to adopt a more “Anglo” sounding name. Still, it would be nice to know.